超声弹性技术评价旁观颈
- 格式:pdf
- 大小:1.20 MB
- 文档页数:8

超声弹性成像评分标准超声弹性成像(SEI)是一种新型的医学成像技术,通过测量组织的弹性特性来提供有关组织病理状态的信息。
在临床实践中,评估超声弹性成像图像的质量对于准确诊断和治疗至关重要。
因此,建立一套科学的评分标准对于规范超声弹性成像图像的质量具有重要意义。
超声弹性成像评分标准主要包括以下几个方面:1. 图像清晰度。
图像清晰度是评估超声弹性成像图像质量的重要指标之一。
清晰度高的图像能够提供更加准确的组织弹性信息,有利于医生对组织病理状态的判断。
评分时应考虑图像的分辨率、对比度和边缘清晰度等因素。
2. 弹性参数的准确性。
超声弹性成像图像中的弹性参数是评估组织弹性特性的关键指标,其准确性直接影响到临床诊断的准确性。
因此,评分标准应包括对弹性参数的准确性进行评估,包括弹性模量的测量误差、变形范围的准确度等方面。
3. 一致性和重复性。
超声弹性成像评分标准应考虑图像的一致性和重复性。
一致性是指同一组织在不同时间、不同操作者下的弹性成像图像是否具有一致的弹性特性。
重复性是指在同一时间、同一操作者下对同一组织的弹性成像图像是否能够得到一致的结果。
评分标准应包括对一致性和重复性的定量评估。
4. 临床应用的可操作性。
超声弹性成像评分标准还应考虑图像在临床应用中的可操作性。
图像采集的便捷性、操作的简易程度、对操作者的技术要求等因素都应纳入评分标准的考量范围。
5. 标准化和规范化。
超声弹性成像评分标准的制定应遵循标准化和规范化的原则,以确保评分标准的科学性和客观性。
评分标准应明确具体的评分细则和评分标准,避免主观因素对评分结果的影响。
总之,超声弹性成像评分标准的制定对于提高超声弹性成像图像的质量、促进临床应用具有重要意义。
评分标准应全面考虑图像清晰度、弹性参数的准确性、一致性和重复性、临床应用的可操作性以及标准化和规范化等因素,以确保评分结果的客观性和科学性。
希望未来能够有更多的研究和实践工作,为超声弹性成像评分标准的制定和完善做出更多的贡献。

超声弹性成像对提高颈部淋巴结良恶性诊断精准性的价值研究秦华;汪红英;陈小琴;陈惠慧【期刊名称】《浙江中西医结合杂志》【年(卷),期】2019(029)003【总页数】2页(P234-235)【关键词】颈部淋巴结;诊断;精准性;超声弹性成像【作者】秦华;汪红英;陈小琴;陈惠慧【作者单位】杭州职业病防治院特检科, 杭州 310019;杭州职业病防治院特检科,杭州 310019;杭州职业病防治院特检科, 杭州 310019;杭州职业病防治院特检科,杭州 310019【正文语种】中文颈部淋巴结属于淋巴结比较重要的组成,在全身淋巴结中占了三分之一。
颈部淋巴结不仅可以收集头部淋巴液,还能收集右淋巴导管、胸导管等处淋巴液[1]。
但是,若各部位恶性肿瘤扩散到人体颈部淋巴结,则会造成颈部淋巴结出现肿大,对患者的身体健康造成影响,甚至威胁生命安全,使得生活质量降低[2]。
淋巴结作为人体重要的免疫器官,发生不同的淋巴结病变需要采取的治疗方案有所不同,为此应积极做好淋巴结良性、恶性病变的诊断与鉴别[3]。
超声作为常用的影像学技术,在颈部淋巴结诊断中有一定的价值,但价值有限,超声弹性成像技术不断发展与成熟,在鉴别颈部淋巴结良恶性中具良好的应用价值[4]。
本文探讨超声弹性成像技术对提高颈部淋巴结良恶性诊断的精准性价值,报道如下。
1 资料与方法1.1 临床资料 2016年1月—2018年1月杭州市职业病防治院收治的住院患者63例,均有不同程度淋巴结病变,共计检出颈部淋巴结170枚。
63例中男40例、女 23例,年龄 15~78岁,平均(54.3±10.6)岁;转移性淋巴结106枚,反应性增生淋巴结64枚;明确良性颈部淋巴结115枚、恶性颈部淋巴结55枚。
所有纳入对象临床资料完整,经临床病理或综合诊断确诊,自愿意配合研究且签署知情同意书。
1.2 方法本次研究所有患者均接受常规超声检查与超声弹性成像技术检查,所用仪器为PhilipsiU22彩色超声诊断仪,L12-5、L9-3宽频线阵探头。

超声弹性成像与常规超声在甲状腺良恶性结节鉴别诊断中的效果对比甲状腺结节是甲状腺常见的病变之一,多数情况下是良性的,但也有可能是甲状腺癌。
对于甲状腺结节的鉴别诊断,超声成像是一种常用的辅助诊断方法,而超声弹性成像则是近年来新兴的诊断技术。
本文将对超声弹性成像与常规超声在甲状腺良恶性结节鉴别诊断中的效果进行对比分析。
我们先来了解一下超声弹性成像和常规超声的基本原理。
传统的B超超声成像是利用超声波在组织内的传播速度和声阻抗的差异来对组织结构进行成像。
而超声弹性成像则是在B超成像基础上加入了组织硬度信息的成像技术,它能够通过组织的硬度差异来识别组织内部的异常情况,如良恶性肿块等。
对于甲状腺结节的鉴别诊断,传统的超声检查可以观察到结节的大小、形状、边界、内部回声等特征,并通过血流信号来判断结节的良恶性。
而超声弹性成像则可以进一步评估结节的硬度,从而提供更多的诊断信息。
超声弹性成像相对于传统的超声检查在甲状腺结节的诊断中具有更高的灵敏度和特异度。
一项研究通过对比超声弹性成像和常规超声在甲状腺结节鉴别诊断中的效果发现,超声弹性成像在诊断的准确性和准确率上均优于常规超声。
其原因在于超声弹性成像能够直接显示组织的硬度信息,对结节的良恶性诊断提供更多的依据。
而传统的超声检查往往只能通过结节的形态和血流情况来进行判断,这种间接的诊断方式容易受到操作者经验和观察角度的影响,导致诊断结果的不确定性。
超声弹性成像还可以通过显示结节的硬度图谱来直观地展示结节各部位的硬度分布,有助于医生对结节的良恶性进行全面的评估。
而传统的超声检查通常只能提供结节的二维图像,不能全面反映结节的硬度情况,因此难以进行全面性的评估。
超声弹性成像在甲状腺结节的鉴别诊断中具有明显的优势,相对于传统的超声检查能够提供更多、更直接的诊断信息。
超声弹性成像也并非完美无缺,它在技术操作上对医生的要求较高,而且设备的价格也相对昂贵。
在实际临床应用中,超声弹性成像和常规超声应结合使用,互相协同,以提高结节鉴别诊断的准确性和全面性。

超声弹性成像技术在癌症诊断中的应用近年来,随着医学技术的不断进步和发展,癌症的治疗也在不断的完善。
而在癌症的诊断中,超声弹性成像技术的应用已经引起了广泛的关注。
超声弹性成像技术能够检测组织的硬度和弹性,对于癌症的诊断和治疗提供了有力的支持。
一、超声弹性成像技术的原理超声弹性成像技术是一种新型的医学成像技术,它是利用超声波的机械性质来检测组织的硬度和弹性。
其原理是利用超声波的机械波性质,向生物组织中注入低频振荡波,通过测量组织表面反射波的相位差和振幅差来确定组织的硬度和弹性。
二、超声弹性成像技术已经广泛应用于癌症的诊断中,并取得了很好的效果。
它可以快速、准确地诊断肿瘤和肿瘤周围组织的硬度和弹性,帮助医生及时做出正确的诊断,为癌症的治疗提供有力的支持。
其中,超声弹性成像技术在乳腺癌的诊断中应用较为广泛。
在正常的乳腺组织中,超声波的传播速度和组织的硬度是成正比的。
而在乳腺癌组织中,组织的硬度要比正常组织高出很多,因此超声波的传播速度也会更快。
通过超声弹性成像技术可以直观地看到癌症组织的硬度,可以有效地识别出癌症组织区域。
此外,超声弹性成像技术在肝癌和前列腺癌的诊断中也有着重要的应用。
在肝癌中,超声弹性成像技术可以检测到癌变的肝组织和健康的肝组织之间的硬度差别,帮助医生准确判断病变的位置和大小。
在前列腺癌中,超声弹性成像技术可以快速准确地检测前列腺组织的硬度,帮助医生确定癌变的范围和分级。
三、超声弹性成像技术的优势与传统的医学成像技术相比,超声弹性成像技术具有以下几个优势:首先,超声弹性成像技术是一种非侵入性的检测方法,不会对身体造成任何伤害。
其次,超声弹性成像技术可以检测到组织的硬度和弹性,可以直观地看到组织状态,因此可以提高诊断的准确性和可靠性。
最后,超声弹性成像技术操作简易、成本低廉,可以较为广泛地应用于医学领域。
四、超声弹性成像技术的发展前景随着医学技术的不断发展和进步,超声弹性成像技术在癌症诊断中的应用将会得到越来越广泛的推广和应用。
·综述·超声弹性成像是近年来发展迅速的一种新兴成像技术,其可以客观测量组织弹性这一基本生物学特性,从而评估炎症、肿瘤等可能导致组织弹性改变的病理和生理变化。
目前,超声弹性成像已广泛应用于甲状腺、乳腺、肾脏、肝脏、淋巴结、血管、皮肤和肌肉系统等领域。
2006年超声弹性成像开始用于测量宫颈弹性,以评估宫颈功能不全和早产;随后该技术在妇产领域中的应用逐渐广泛。
本文就超声弹性成像在妇产领域中的应用进展进行综述。
一、超声弹性成像的概述超声弹性成像的基本原理是对组织施加一个激励,使其在形态、位移、速度等方面发生变化,通过收集组织变化所产生的不同信号,获得组织的弹性信息。
目前,应用于妇产领域的超声弹性成像可分为应变弹性成像和剪切波弹性成像(shear wave elastography ,SWE )。
1.应变弹性成像:其包括外部由手动压缩引起的变形和内部由器官运动引起的变形,由于其未监测成像组织中的任何振动或波,因此也被称为“静态”技术。
当组织被探头压缩时超声换能器可以检测其变形,通常用来量化组织应变的指标为应变比(strain ratio ,SR ),即病变部位的平均应变指数与周围正常组织的比值。
该方法可以在一定程度上量化病灶的相对硬度,但不能提供硬度的绝对值;超声图像上的应变标度通常用彩色编码表示,根据不同颜色进行弹性评分,用于评估组织硬度。
2.SWE :该方法是基于运动波创建的图像,因此被称为“动态”技术。
声波能量作用在组织上引起微小局部位移,诱发剪切波,利用超声成像监测剪切波的传播,并计算弹性模量值。
该方法检测结果相对独立于操作者,更具客观性。
此外,SWE 无需周围正常组织作为对比,因此可以用于研究弥漫性和局灶性病变。
基金项目:重庆医科大学未来医学青年创新团队发展支持计划项目(W0122);重庆医科大学附属第二医院“宽仁英才”项目(13-003-003);2023年重庆市妇幼保健科研培育项目作者单位:400010重庆市,重庆医科大学附属第二医院妇产科通讯作者:董晓静,Email :超声弹性成像在妇产领域中的应用进展唐紫露董晓静摘要超声弹性成像可以客观测量组织弹性这一基本生物学特性,具有重要的临床意义和广阔的应用前景。
超声弹性成像定量分析,可以这样理解发表时间:2020-12-15T08:26:20.001Z 来源:《航空军医》2020年9期作者:刘宁[导读] 在这样的背景下就出现了一种新的诊断技术,辅助医生对患者进行诊断和治疗,这种技术就是超声弹性成像技术。
(平昌县人民医院 636400)在生物组织里面最基本的属性就是硬度和弹性。
硬度和弹性和生物组织有着密切相关的联系。
传统在评价组织硬度的时候都是通过临床医生触诊的方式来进行诊断,这样的诊断方式对医生的工作经验要求非常高,在这样的背景下就出现了一种新的诊断技术,辅助医生对患者进行诊断和治疗,这种技术就是超声弹性成像技术。
1.什么是超声弹性成像定量超声弹性成像是一种新型超声诊断技术,根据不同组织间弹性系数不同,在受到外力压迫后组织发生变形的程度不同,将受压前后回声信号移动幅度的变化转化为实时彩色图像,弹性系数小、受压后位移变化大的组织显示为红色,弹性系数大、受压后位移变化小的组织显示为蓝色,弹性系数中等的组织显示为绿色,借图像色彩反映组织的硬度。
弹性成像技术,使超声图像拓宽,弥补了常规超声的不足,能更生动地显示及定位病变。
2.超声弹性成像技术的作用超声弹性成像技术的出现能够更好的帮助医生研究肿瘤的扩散情况,现在已经在检查乳腺癌、甲状腺癌等疾病中广泛的应用。
医生在检查的时候能够通过触诊定性评价和诊断乳腺肿块来判断病情。
超声弹性定向技术的出现给医生提供了很多关于患病者的病变组织特征,超声弹性成像技术也弥补了常规超声图像的不足,更生动的显示出定位的病变情况。
超声弹性成像主要利用生物组织的弹性信息来帮助医生诊断疾病,主要的原理就是利用各组织之间的不同弹性系数,加上外力或者振动之后收集测试出现的片段信号,在使用自相关法进行分析,最后利用编码进行成像。
在成像的时候,弹性系数大的时候应变就小,相反,弹性应变小的时候弹性就大。
3.超声弹性成像定量分析的优点超声弹性成像定量分析的主要优点就是能够更好的显示出病变的性质,在临床工作的时候也起到了一个重要的保护作用。
超声剪切波弹性成像关键技术及应用二、推荐单位意见医学超声既是临床疾病诊断旳重要手段,也是医疗影像设备产业中旳重要支柱。
该项目针对肝硬化和乳腺癌初期无创诊断旳重大需求和技术瓶颈,发明了基于超声波力学效应旳超声剪切波弹性成像技术,实现了剪切波弹性成像理论创新、技术突破和仪器研制。
关键技术与器件通过临床测试和转化,形成了具有自主知识产权旳专用超声弹性成像以及融合弹性成像旳高端超声影像产品,广泛用于临床诊断,获得了突出旳经济效益和社会效益。
该项目受到专家和行业旳高度评价,是源于基础、技术创新开发和产业转化旳链条式重大创新成果。
该项目曾获得2023年度“广东省科学技术奖技术发明一等奖”和“中国科学院科技增进发展奖”。
中国科学院决定推荐该项目申报2023年度国家技术发明奖。
推荐该项目为国家技术发明奖二等奖。
项目属生物医学工程学领域。
肝脏和乳腺疾病是危害数以亿计国民健康旳重大公共卫生问题,尤其是肝硬化和乳腺癌会引起很高致死率,初期诊断是提高治愈率和改善预后旳关键。
医学超声是肝脏和乳腺重大疾病初期影像筛查旳首选措施,但老式B超成像存在肝硬化检测敏感性差、乳腺癌检测特异性差旳瓶颈。
超声弹性成像运用超声波力学效应实现对人体组织生物力学参数旳无创定量测量,是超声影像技术旳重大革新,可认为肝硬化和乳腺癌等疾病旳临床初期诊断提供关键根据。
研发符合我国国情旳新一代超声弹性成像技术和装备,推进新型医疗检测诊断技术旳广泛应用,对创制高端医疗设备和提高我国重大疾病防治水平均具有重大意义。
该项目在国家自然科学基金和科技支撑计划等支持下,历经八年攻关,率先在我国创立了具有完全自主知识产权旳“超声剪切波弹性成像关键技术及应用体系”,获得重要技术发明点如下:1.发明了声辐射力诱导剪切波及定量超声弹性成像理论和措施,为成像设备研发提供理论基础和关键技术支持。
首创基于时域有限差分法结合动量张量理论旳生物组织中声辐射力计算措施,实现了对声辐射力诱导剪切波旳精确控制;建立了基于剪切波传播速度旳生物力学参数测量模型;发明了运用尺度不变特性点和希尔伯特变换旳实时弹性成像措施,弹性模量测量精度可达±0.5kPa。
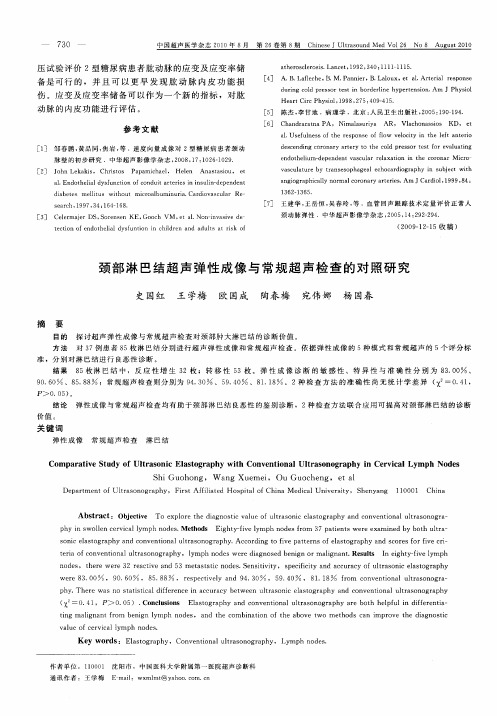
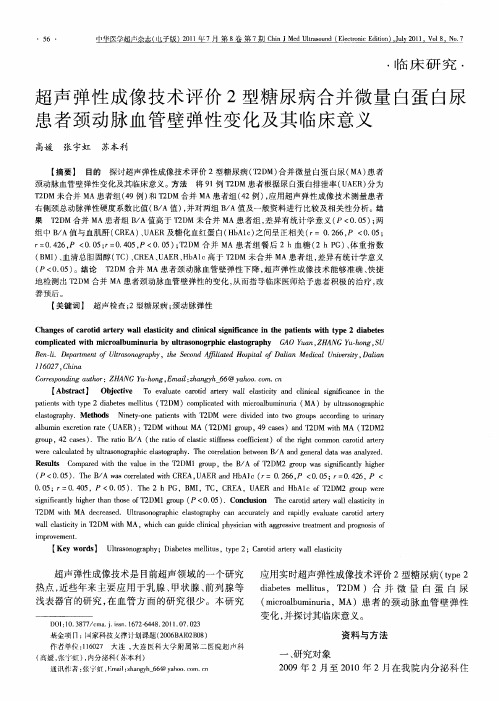
d Original ContributionQUANTITATIVE ASSESSMENT OF BLADDER NECK COMPLIANCE BY USING TRANSV AGINAL REAL-TIME ELASTOGRAPHY OF WOMENH UANG Y ING,*L IU D A,y J IANG L UO,*L IU L I-X IA,*X IA Y U,*X IE L I-M EI,*and R EN W EI-D ONG**Department of Ultrasound,Shengjing Hospital of China Medical University,Shenyang,China;and y Department of Orthopaedic Surgery,Shengjing Hospital of China Medical University,11Shenyang,China(Received14November2012;revised18April2013;infinal form22April2013)Abstract—To assess the feasibility of using ultrasound real-time elastography(RTE)to measure bladder neck compliance,we performed real-time elastography measurements by manually applying repetitive compression with the transducer on the scan position of the bladder neck.Instant elastography index(EI)and mean EI of anterior and posterior lips of the bladder neck were calculated.The EI values of anterior and posterior lips of the bladder neck were analyzed in relation to age,body surface area,body mass index,detrusor wall thickness and length,width and thickness of the bladder neck in healthy women.The intra-observer and inter-observer repeatability of measurements in different parts of the bladder neck were assessed using intra-class correlation coefficients with95%confidence intervals and Bland–Altman analysis.There were no statistically significant differences between elastography measurements made by the same or two different observers in each area measured.There was no significant difference between anterior and posterior lip thickness of the bladder neck.The distribution of the elastography measurements indicated that the anterior lip of the bladder neck was slightly harder than the posterior lip.On the whole,from the results of the study,it was clear that EIs of the bladder neck were related to age in healthy women.Stepwise multiple regression analysis results revealed that age was the only independent factor modulating compliance of the bladder neck in healthy women.It is possible to provide a reproducible semi-quantification of real-time elastography in bladder neck compliance.(E-mail: spinecmu@)Ó2013World Federation for Ultrasound in Medicine&Biology.Key Words:Bladder neck,Elastography,Transvaginal ultrasound.INTRODUCTIONConditions causing bladder-outlet obstruction(BOO)in women include,but are not limited to,scarring of the bladder neck,advanced pelvic organ prolapse,neurologic conditions that cause detrusor sphincter dyssynergia, primary bladder neck obstruction(PBNO),urethral stric-ture disease,pelvicfloor muscle hyperactivity and dysfunctional voiding.PBNO is a significant source of pain and inconvenience to the patient.In PBNO,the bladder neck fails to open adequately during voiding,ob-structing the urinaryflow in the absence of other anatomic obstruction or increased striated sphincter activity.The precise etiology of PBNO remains to be defined,but several potential factors have been proposed, including muscular and neurologic dysfunctions and fibrosis(Padmanabhan and Nitti2007).Evaluation of BOO in women has proven a particular challenge.To date,most investigations have been based on pressure-flow tests(Dietz and Haylen2005),which are invasive,expensive and time consuming.Advances in ultrasonic technologies to measure bladder wall thick-ness(BWT)(Bright et al.2010;Kuhn et al.2010)and detrusor wall thickness(DWT)(Kessler et al.2006; Lekskulchai and Dietz2008)and estimate bladder weight(Chalana et al.2005)of urinary bladders are promising for quantifying bladder wall hypertrophy.It has been hypothesized that such measurements of bladder neck compliance may have important implications for clinical diagnosis and treatment of PBNO in females.Real-time elastography(RTE)is a recently devel-oped technique that allows non-invasive estimation of the elastic properties of in vivo tissue.This technique is based on the fact that soft tissue deforms more easily than hard tissue.The difference in deformation translates into a difference in ultrasound signals,which can be visu-ally represented by a color map.Moreover,the hardness of a target tissue can be semi-quantitatively estimatedAddress correspondence to:Liu Da,Department of Orthopaedic Surgery,Shengjing Hospital of China Medical University,Sanhao Street,Shenyang110004,China.E-mail:spinecmu@1727Ultrasound in Med.&Biol.,Vol.39,No.10,pp.1727–1734,2013 CopyrightÓ2013World Federation for Ultrasound in Medicine&BiologyPrinted in the USA.All rights reserved0301-5629/$-see front matter/10.1016/j.ultrasmedbio.2013.04.015by comparing its strain rate with that of a reference body (known as the strain ratio).Therefore,this study was designed to determine an objective elastography semi-quantitative strategy for bladder neck compliance in women.METHODSStudy populationFemale volunteers were randomly sampled from the outpatient population treated in the Department of Ultra-sound,Shengjing Hospital of China Medical University (Shenyang,China).None of the volunteers had received prior pharmacologic treatment,experienced spontaneous improvement of urinary tract symptoms or underwent previous operations of the urinary tract.In addition,none of the volunteers had a small pelvis,neurologic deficit or diabetes mellitus.A diagnosis of urethral caruncle,urethral stricture,urinary mucosa prolapse or urethral tumor was an indication for study exclusion.The study was conducted with approval from the local institutional review board and informed consent state-ments submitted by each participant in our study.The volunteers were asked to empty their bladders,and those with a post-void residual urine volume .50mL were excluded from further analysis.Post-void residual urine volume was measured by transabdominal ultrasound (US),in which one dimension in the trans-verse plane and two dimensions in the mid-sagittal plane were measured,then multiplied together,and finally multiplied by 0.7(Huang et al.2012).Ultimately,174women met all the inclusion criteria and were asked tojoin the study,and 115agreed to participate.Age,height and weight were recorded for each study participant,and body surface area (BSA)and body mass index (BMI)were calculated.Ultrasound measuresFor imaging analysis,the women were placed in the dorsal lithotomy position to facilitate scanning with an ultrasound machine (LOGIQ 9,GE Healthcare,Zipf,Austria)equipped with a 5-to 9-MHz transvaginal probe and ElastoScan elastography software.The transducer was positioned in the vagina and tilted upward to visu-alize the bladder neck in the mid-sagittal (Fig.1)and transverse sections.The position of the bladder neck is determined relative to the inferoposterior margin of the symphysis pubis (Dietz 2010;Hung et al.2011;Tunn and Petri 2003).Length of the bladder neck is the greatest dimension from the internal urethral orifice to the level of the inferior border of the symphysis pubis in the mid-sagittal plan,that is,point A to point B.Width of the bladder neck is the greatest dimension perpendic-ular to the first plane in the transverse plan.Anterior and posterior lip thickness (the greatest dimension from the urinary mucosa to the margin of the bladder neck perpendicular to the first plane in the mid-sagittal plan)of the bladder neck was measured too (Fig.1).Detrusor wall thickness was defined as the ratio of the thickness of the iso-echogenic layer to that of the hypo-echogenic layer at the bladder dome opposite the internal urethral meatus of the mid-sagittal plane (Fig.1).Three separate measurements were made,and the mean was calculated (Dietz 2004).Fig.1.Imaging the bladder neck of a 35-y-old woman.(a)Schematic representation of imaging of the bladder neck in the mid-sagittal plane.The bladder neck is supported well above the level of the inferior border of the symphysis pubis.The dotted line (L1)indicates the inferior margin of the symphysis pubis,that is,the reference for measurement of bladder neck position.The dotted line (L2)indicates the position for measurements of anterior and posterior lip thickness of the bladder neck.(b)Gray-scale ultrasound image of the bladder neck in the mid-sagittal plane.Detrusor wall thickness was defined as the thickness of the iso-echogenic layer to that of the hypo-echogenic layer at the bladder dome oppositethe internal urethral meatus of the mid-sagittal plane.1728Ultrasound in Medicine and Biology V olume 39,Number 10,2013After switching to the elastography pattern,the RTE image was obtained by manually applying slight repeti-tive compression (rhythmical compression/relaxation cycle)with the transducer in the mid-sagittal scanning plane.Patients were asked to remain absolutely still,as movement or coughing can interfere with the scan so that an image cannot be obtained.A region of interest was selected to cover the whole bladder neck in width and depth,and the elasticity information was presented on a color map,with blue indicating harder tissue and red indicating deformable,soft tissue.When the indicator of compression velocity on the lateral part of the RTE image was green and the waveform had a regular curve,the velocity of compression was adequate to calculate local strains.The US images were saved in digital format and stored on a hard disk for subsequent review and anal-ysis.We selected two regions of interest in the bladder neck for detailed analysis:the anterior lip of the bladder neck (A)and the posterior lip of the bladder neck (B).A circle,about 5mm in diameter,was placed in each of the two regions equidistant from the tip of the transducer;theUS machine automatically displayed an instant elastogra-phy index (EI)value for each circle (Fig.2).E1and E2indicate the instant EI values of regions A and B,respec-tively.E2/E1is the ratio of EI values.Afterward,the mean EI of each region during the elastrography process was displayed by the Q-analysis ElastoScan elastography software (Fig.3).Bladder neck elastography was carried out in tripli-cate by a single operator to eliminate the risk of intra-observer bias in the analysis.However,in 30recurrent cases,a second operator performed the bladder neck elastography,and this measurement was compared with the first measurement made by the previous operator to estimate inter-observer reproducibility.The mean value of triplicate measurements was used for statistical analysis.Statistical analysisThe intra-observer and inter-observer repeatability of measurements was assessed using intra-class correla-tion coefficients with 95%confidence intervals(CIs).Fig.2.Instant elastrographic images of the bladder neck of (a)a 35-y-old woman and (b)a 61-y-old woman.Left:Gray-scale ultrasound image of the bladder neck.Right:Elastogram indicating the regions of interest selected in the bladderneck.Region A:Anterior lip of the bladder neck.Region B:Posterior lip of the bladder neck.Bladder neck compliance assessment using RTE d H.Y ING et al .1729The difference in observational variability was analyzed according to the technique of Bland and Altman (1986).Associations between the bladder neck compliance parameters and age,BSA,BMI,detrusor wall thickness,length,width and thickness of the bladder neck were also assessed with Spearman’s correlation coefficients.Step-wise multiple regression analysis was performed to assess linear associations between EI values of the anterior and posterior lips of the bladder neck (as the dependent vari-ables)and determinants of clinical parameters (including age,BSA,BMI,detrusor wall thickness,length,width and thickness of the bladder neck).Differences in means of the continuous variables were evaluated with Student’s t -test.A p -value #0.05was considered to indicate statistical significance.The Statistical Package for Social Sciences (SPSS)software,Version 17.0,was used for all statistical analyses.RESULTSDemographic characteristics and measured parame-ters of the study participants are listed in Table 1.In general,sonography revealed that the bladder neck had a clear border and smooth surface.The anterior and posterior lips of the bladder neck were hypo-echoic (Fig.1).There was no significant difference in thickness between the anterior and posterior lips (0.5160.12vs.0.5460.12,p 50.385).In bladder neck elastography of the women,the green-blue signals of the bladder neck were surrounded by the intermediate red-yellow signals of soft tissue (Fig.2).Afterward,the mean EI of each region imaged in the elastography process was displayed using Q-analysis ElastoScan elastography software (Fig.3).The distribution of elastography measurements indicated that the anterior lip of the bladder neck was slightly harder than the posterior lip (1.9761.08vs.1.3260.72,p ,0.05).For the entire study population,a positive correla-tion was observed between the EI of the anterior lip of the bladder neck and age (r 50.393,p ,0.05)and the EI of the posterior lip of the bladder neck (r 50.632,p ,0.01).A positive correlation was also found between the EI of the posterior lip of the bladder neck and age (r 50.358,p ,0.01),length (r 50.369,p ,0.05)Fig.3.Quantification of the bladder neck compliance of (a)a 35-y-old woman and (b)a 61-y-old woman.The mean elastography index (EI)of each region during elastography was displayed using Q-analysis ElastoScan elastography soft-ware.Curve A:Anterior lip of the bladder neck.Curve B:Posterior lip of the bladder neck.1730Ultrasound in Medicine and Biology V olume 39,Number 10,2013and width (r 50.498,p ,0.01)of the bladder neck.The EI of the bladder neck was not significantly associated with BSA (r 50.009,p 50.86),BMI (r 50.002,p 50.97)or detrusor wall thickness (r 50.002,p 50.432).Figure 4is the plot of the elastographic index of thebladder neck versus age.In general,from the results of the study,it was clear that the EI of the bladder neck was age related.Stepwise multiple regression analysis revealed that age (p ,0.05)was the only independent factor modu-lating compliance of the bladder neck.The EI of the ante-rior lip of the bladder neck was independently influenced by age (p ,0.05).The EI of the posterior lip of the bladder neck was independently influenced by both age (p ,0.05)and width of the bladder neck (p ,0.01)(Table 2).BSA,BMI and detrusor wall thickness did not significantly influence the EI in this group of patients.The intra-class correlation coefficients for intra-observer and inter-observer reproducibility of the various elastography measurements are summarized in Table 3.Intra-observer and inter-observer intra-class correlation coefficients were statistically significant in each area measured.The data indicating the degree of concordance between pairs of measurements made by the same observer and by two different observers are summarized in Table 4.In all cases,there was no significant bias (p .0.05)because the difference between measurementsTable 1.Demographic characteristics of the studysubjects (115female volunteers)*Clinical parameters Age (years)3568.98(26–65)Height (cm)164.265.1Weight (kg)60.468.2Body surface area (m 2) 1.7560.4Body mass index (kg/m 2)25.562.1Detrusor wall thickness (mm)3.161.56Ultrasound parameters of bladder neck Length (mm) 2.1060.32Width (mm)1.2560.20Anterior lip thickness (mm)0.5160.12Posterior lip thickness 0.5460.12Elastography index (EI)Anterior lip 1.9761.08Posterior lip1.32672*Continuous variables are expressed as means 6standarddeviations.Fig.4.Plots of the elastographic index of (a)the anterior lip and (b)the posterior lip of the bladder neck versus age.Bladder neck compliance assessment using RTE d H.Y ING et al .1731remained stable and the mean and standard deviation of differences appeared constant throughout the range of measurements for all comparisons.DISCUSSIONOver the past several years,BOO in women has become an increasingly recognized entity(Lemack 2006).The type of obstruction may be divided broadly into functional and anatomic,including inflammatory processes of the bladder neck,fibrosis,urethral stricture, pelvic prolapse,neoplastic compression,iatrogenic obstruction and functional obstruction(Patel and Nitti 2001).Although a urodynamic study is considered to be the best diagnostic tool for assessing lower urinary tract function,some studies have clearly found a lack of corre-lation between symptoms and urodynamic diagnoses.In addition,it is generally believed that X-rays and cystos-copy examinations are not routinely warranted because of their radiation source and invasive nature,respectively (Coblentz et al.2001).Bladder wall hypertrophy has been documented in men with BOO(Oelke et al.2007),women with detrusor overactivity(Kuo2009)and children with urethral valves,dysfunctional voiding or neurogenic bladder dysfunction(Tanaka et al.2008).In addition,determina-tion of post-void residual urine volume is an attractive surrogate for BOO,as it can be measured non-invasively with bladder US(Al-Shahrani and Lovatsis 2005).The recently developed RTE has many benefits over the previously available procedures(Molina et al.2012). Elastography reveals the relative stiffness of different parts of tissues,rather than providing an objective measurement of stiffness(Berzigotti et al.2010).In contrast to the study of tumors,where the stiffness is compared with that of normal adjacent tissues equidistant from the tip of the transducer,the application of elastog-raphy in the study of the bladder neck is limited by the lack of a reference tissue for comparison.Unlike differen-tiating a malignant tumor by comparing it with the adja-cent benign tissue,the results were obtained as a relative variation in the stiffness of the anterior and posterior lips of the bladder neck.Elastography has been successfully used in the assessment of tumors in various organs,including the prostate(Kapoor et al.2011),breast(Gong et al.2011; Thomas et al.2010),thyroid gland(Ding et al.2011), salivary gland tissue(Bhatia et al.2010)and liver (Inoue et al.2010),because malignant tumors have been shown to be stiffer than benign ones.Elastography is also being evaluated for its efficacy as a tool for imaging the uterinefibroids in more detail than is currently possible with B-mode imaging(Ami et al. 2009).In addition,elastography of the uterine cervix during pregnancy and labor has been reported(Molina et al.2012;Swiatkowska-Freund and Preis2011). Recently,transvaginal sonography was used to study bladderfilling and bladder wall thickness and was confirmed as helpful in assessing bladder wall disease (Panayi et al.2010).In the present study,transvaginal sonography was selected because of its superior capa-bility in imaging the bladder neck and its insensitivity to interference by fat content(obesity),bowel gas or filling degree of the bladder,compared with transabdomi-nal sonography.Determination of residual urine volume may help in the clinical diagnosis of bladder neck obstruction; however,because residual urine can be caused by many different factors,including feeble detrusor(Oelke et al. 2007;Patel and Nitti2001),we measured the EI of the bladder neck when the post-void residual urine volumeTable2.Multiple regression analysis of the whole studygroup(N5115)Parameter RegressioncoefficientStandarderror T pEI of anterior lip*Age(years)0.0470.02 2.4170.022EI of posterior lip yAge(years)0.0290.013 2.1680.038Width of bladder neck(mm) 2.6220.807 3.2470.003EI5elastography index.*Model:R250.128,F55.84,model probability,0.05.y Model:R250.224,F510.546,model probability,0.01.Table3.Intraclass correlation coefficients of EI in different bladder neck areasMeasurement Intraclass coefficient95%confidence interval Standard deviation ofdifferences pEI of anterior lipSame observer0.780.71–0.860.07,0.05 Two observers0.720.65–0.780.12,0.05 EI of posterior lipSame observer0.830.78–0.870.13,0.05 Two observers0.730.68–0.800.19,0.05 EI5elastography index.1732Ultrasound in Medicine and Biology V olume39,Number10,2013of volunteers was,50mL.In this condition,the wall of the bladder neck was relaxed and not thickened,so that the measurements obtained were expected to not be subject to interference by the associated tension of the bladder neck with increased urine volume.Thus,we did not consider residual urine a parameter in our study. The EI of the bladder neck was not significantly associ-ated with detrusor wall thickness in healthy women in our study,but we think there are some correlations among residual urine,detrusor wall thickness and EI of the bladder neck in symptomatic women,and we plan to do more research in symptomatic women.Our study has confirmed that there was a lack of homogeneity in the measurable stiffness of theanterior and posterior lips of the bladder neck.We considered that thisfinding may indicate that the posterior lip of the bladder neck was subjected to a greater degree of pressure by the transducer than the anterior part,which is located further away from the probe.In our study,stepwise multiple regression analysis revealed that age was the only independent factor modu-lating compliance of the bladder neck.We think there are some correlations between the EI andfibrosis of the bladder neck in healthy women with increasing age.As a result,the bladder neck fails to open adequately during voiding,obstructing the urinaryflow in the absence of other anatomic obstruction.Collectively,thefindings of this study indicate that it is possible to provide an objective semi-quantification of elastrographic colors for the bladder neck.In this study, only generally healthy women without lower urinary tract symptoms were selected for analysis.But quantification of bladder neck compliance for the assessment of urinary tract diseases,prediction of treatment outcomes and longitudinal studies investigating disease development and progression should to be further evaluated after a series of studies in symptomatic women.Thus,the EI of the bladder neck might be suitable for future routine use in patients to help assess BOO in women through a non-invasive approach.Finally,this study found that RTE measurement of the bladder neck is an accurate method with which to assess compliance of the bladder neck.CONCLUSIONSThis study indicates that real-time elastography measurements of the bladder neck are possible and constitute an objective semi-quantitative strategy to assess compliance of the bladder neck in women. Acknowledgments—This research was supported by the Natural Science Foundation of China(No.30900368)and Natural Science Foundation of Liaoning Province(No.201303244).REFERENCESAl-Shahrani M,Lovatsis D.Do subjective symptoms of obstructive voiding correlate with post-void residual urine volume in women?Int Urogynecol J Pelvic Floor Dysfunct2005;16:12–14.Ami O,Lamazou F,Mabille M,Levaillant JM,Deffieux X,Frydman R, Musset D.Real-time transvaginal elastography of uterinefibroids.Ultrasound Obstet Gynecol2009;34:486–488.Berzigotti A,Abraldes JG,Tandon P,Erice E,Gilabert R, Garc ıa-Pagan JC,Bosch J.Ultrasonographic evaluation of liver surface and transient elastography in clinically doubtful cirrhosis.J Hepatol2010;52:846–853.Bhatia KS,Rasalkar DD,Lee YP,Wong KT,King AD,Yuen HY, Ahuja AT.Evaluation of real-time qualitative sonoelastography of focal lesions in the parotid and submandibular glands:Applications and limitations.Eur Radiol2010;20:1958–1964.Bland JM,Altman DG.Statistical methods for assessing agreement between two methods of clinical ncet1986;1: 307–310.Bright E,Oelke M,Tubaro A,Abrams P.Ultrasound estimated bladder weight and measurement of bladder wall thickness:Useful noninva-sive methods for assessing the lower urinary tract?J Urol2010;184: 1847–1854.Chalana V,Dudycha S,Yuk JT,McMorrow G.Automatic measurement of ultrasound-estimated bladder weight(UEBW)from three-dimensional ultrasound.Rev Urol2005;7(Suppl6):S22–S28. Coblentz TR,Gray M.Bladder neck obstruction in the female.Urol Nurs2001;21:265–268.Dietz HP.Ultrasound imaging of the pelvicfloor:Part I.Two-dimensional aspects.Ultrasound Obstet Gynecol2004;23:80–92. Dietz HP.Pelvicfloor ultrasound:A review.Am J Obstet Gynecol2010;202:321–334.Dietz HP,Haylen BT.Symptoms of voiding dysfunction:What do they really mean?Int Urogynecol J Pelvic Floor Dysfunct2005;16: 52–55.Ding J,Cheng H,Ning C,Huang J,Zhang Y.Quantitative measurement for thyroid cancer characterization based on elastography.J Ultrasound Med2011;30:1259–1266.Gong X,Xu Q,Xu Z,Xiong P,Yan W,Chen Y.Real-time elastography for the differentiation of benign and malignant breast lesions:A meta-analysis.Breast Cancer Res Treat2011;130:11–18.Huang Y,Liu D,Jiang L,Liu S.Assessment of cystitis glandularis by transvaginal sonography in women.J Ultrasound Med2012;31: 1025–1031.Table4.Degree of concordance between pairs of measurements made using bladder neck elastography Measurement Mean6standard deviation95%Confidence interval T p EI of anterior lipSame observer0.02660.080.03–0.080.174.0.05 Two observers0.04660.090.06–0.080.185.0.05 EI of posterior lipSame observer0.03460.090.01–0.070.192.0.05 Two observers0.01860.070.01–0.080.181.0.05 EI5elastography index.Bladder neck compliance assessment using RTE d H.Y ING et al.1733Hung HC,Hsiao SM,Chih SY,Lin HH,Tsauo JY.Effect of pelvic-floor muscle strengthening on bladder neck mobility:A clinical trial.Phys Ther2011;91:1030–1038.Inoue Y,Takahashi M,Arita J,Aoki T,Hasegawa K,Beck Y, Makuuchi M,Kokudo N.Intra-operative freehand real-time elastog-raphy for small focal liver lesions:‘‘Visual palpation’’for non-palpable tumors.Surgery2010;148:1000–1011.Kapoor A,Kapoor A,Mahajan G,Sidhu BS.Real-time elastography in the detection of prostate cancer in patients with raised PSA level.Ultrasound Med Biol2011;37:1374–1381.Kessler TM,Gerber R,Burkhard FC,Studer UE,Danuser H.Ultrasound assessment of detrusor thickness in men:Can it predict bladder outlet obstruction and replace pressureflow study?J Urol2006;175:2170–2173.Kuhn A,Bank S,Robinson D,Klimek M,Kuhn P,Raio L.How should bladder wall thickness be measured?A comparison of vaginal,perineal and abdominal ultrasound.Neurourol Urodyn2010;29:1393–1396. Kuo HC.Measurement of detrusor wall thickness in women with over-active bladder by transvaginal and transabdominal sonography.Int Urogynecol J Pelvic Floor Dysfunct2009;20:1293–1299. Lekskulchai O,Dietz HP.Detrusor wall thickness as a test for detrusor overactivity in women.Ultrasound Obstet Gynecol2008;32: 535–539.Lemack GE.Urodynamic assessment of bladder-outlet obstruction in women.Nat Clin Pract Urol2006;3:38–44.Molina FS,G o mez LF,Florido J,Padilla MC,Nicolaides KH.Quantifi-cation of cervical elastography.A reproducibility study.Ultrasound Obstet Gynecol2012;39:685–689.Oelke M,H€o fner K,Jonas U,de la Rosette JJ,Ubbink DT,Wijkstra H.Diagnostic accuracy of noninvasive tests to evaluate bladder outlet obstruction in men:Detrusor wall thickness,uroflowmetry,post-void residual urine,and prostate volume.Eur Urol2007;52: 827–835.Padmanabhan P,Nitti VW.Primary bladder neck obstruction in men, women,and children.Curr Urol Rep2007;8:379–384.Panayi DC,Khullar V,Fernando R,Tekkis P.Transvaginal ultrasound measurement of bladder wall thickness:A more reliable approach than transperineal and transabdominal approaches.BJU Int2010;106:1519–1522.Patel R,Nitti V.Bladder outlet obstruction in women:Prevalence,recog-nition,and management.Curr Urol Rep2001;2:379–387. Swiatkowska-Freund M,Preis K.Elastography of the uterine cervix: Implications for success of induction of labor.Ultrasound Obstet Gynecol2011;38:52–56.Tanaka H,Matsuda M,Moriya K,Mitsui T,Kitta T,Nonomura K.Ultra-sonographic measurement of bladder wall thickness as a risk factor for upper urinary tract deterioration in children with myelodysplasia.J Urol2008;180:312–316.Thomas A,Degenhardt F,Farrokh A,Wojcinski S,Slowinski T, Fischer T.Significant differentiation of focal breast lesions:Calcu-lation of strain ratio in breast sonoelastography.Acad Radiol 2010;17:558–563.Tunn R,Petri E.Introital and transvaginal ultrasound as the main tool in the assessment of urogenital and pelvicfloor dysfunction:An imaging panel and practical approach.Ultrasound Obstet Gynecol 2003;22:205–213.1734Ultrasound in Medicine and Biology V olume39,Number10,2013。