
Bi-directional cavopulmonary shunt:is accessory pulsatile ˉow,
good or bad?q
Henry J.C.M.van de Wal *,Ruth Ouknine,Daniel Tamisier,Marilyne Le
?vy,Pascal R.Vouhe
?,Francine Leca Department of Thoracic and Cardiovascular surgery,Laennec Hospital,Paris,France Received 21September 1998;received in revised form 30April 1999;accepted 19May 1999
Abstract
Objective :Evaluation of the effect and long-term outcome of accessory pulsatile blood ˉow versus classical bi-directional cavopulmonary
connection (BCPC).Methods :Retrospective review of the medical and surgical records.Results :Two-hundred and ?ve patients (119boys,86girls)underwent BCPC from 1990to 1996.Accessory pulsatile ˉow was present in 68%,ˉow being maintained through the pulmonary trunc in 46%,systemic-to-pulmonary artery shunt in 13%and mixed in 7%,or patent ductus arteriosus in 2%.Patients with accessory pulsatile ˉow had lower hospital mortality (3%versus 5%),while mean pulmonary artery pressure (14.1versus 12.6mmHg P 0:050)and increase of oxygen saturation (12.4versus 8.7,P 0:034)were signi?cantly higher.The period of arti?cial ventilation (1.9day)and ICU stay (6days)did not differ for both https://www.doczj.com/doc/0012788814.html,te mortality was higher following accessory pulsatile ˉow (6%versus 1%).At late follow-up patients with accessory pulsatile ˉow had signi?cantly higher oxygen saturation (mean 85^4%,versus 79^4%;P #0:005).If subsequent completion of Fontan is considered the optimal palliation and subsequent systemic to pulmonary artery shunt,arteriovenous ?stula and transplantation is considered a failure,patients with accessory pulsatile ˉow had signi?cantly more and earlier completion of the Fontan procedure (mean 1:7^2:4years,versus 2:7^4:4years;P 0:008).Survival is not inˉuenced by age at bi-directional cavopulmonary shunt surgery,left or right functional ventricular anatomy or previous palliative surgery.One patient with accessory pulsatile ˉow developed systemic-to-pulmonary collateral's eventually requiring lobectomy.Conclusion :Despite two different initial palliative techniques the outcome was not signi?cantly different.Accessory pulsatile blood ˉow appeared not to be a contra-indication for a completion Fontan procedure.Moreover,the data suggest that after accessory pulsatile ˉow can safely be performed,at late follow-up oxygen saturation is higher,while,signi?cantly more and earlier completion of Fontan occurred.Age at bi-directional cavopulmonary shunt,basic left or right ventricular anatomy or previous palliative surgery did not inˉuence survival.q 1999Elsevier Science B.V.All rights reserved.
Keywords:Functionally single ventricle;Glenn procedure;Pulsatile blood ˉow;Follow-up
1.Introduction
Bi-directional superior cavopulmonary connection (BCPC)is a widely used method of providing pulmonary blood ˉow in patients with complex congenital cardiac malformations characterised by univentricular atrio-venous connections [1,2,3].Besides being used as an intermediate stage between systemic-to-pulmonary artery shunt or pulmonary artery band and Fontan procedure it has also been advocated as initial palliation in patients who have
progressed beyond the neonatal period without the need for previous intervention [4,5].
Accessory pulsatile blood ˉow is de?ned as the presence of either a systemic-to-pulmonary artery shunt,a patent ductus arteriosus or a patent right ventricular outˉow https://www.doczj.com/doc/0012788814.html,rmation on the use of accessory pulsatile blood ˉow in young infants is limited,few reports have addressed the issue of whether or not to leave an additional source of pulmonary blood ˉow at the time of BCPC [3,6,7].Concerns remain about peri-operative morbidity and mortality and about post-operative systemic arterial oxy-genation in very young patients [5,8].
We have therefore reviewed our experience and long-term outcome of BCPC with and without accessory pulsatile ˉow.
European Journal of Cardio-thoracic Surgery 16(1999)
104±110
1010-7940/99/$-see front matter q 1999Elsevier Science B.V.All rights reserved.PII:S1010-7940(99)00205-5
q
Presented at the 12th Annual Meeting of the European Association of Cardio-thoracic Surgery,Brussels,Belgium,September 20±23,1998.*Corresponding author.Nieuwe Hescheweg 104,NL 5342EE Oss,The Netherlands.Tel.:131-412-623213.
E-mail address:vandewal@wxs.nl,(H.J.C.M.van de Wal)
2.Patients and methods
2.1.Patients
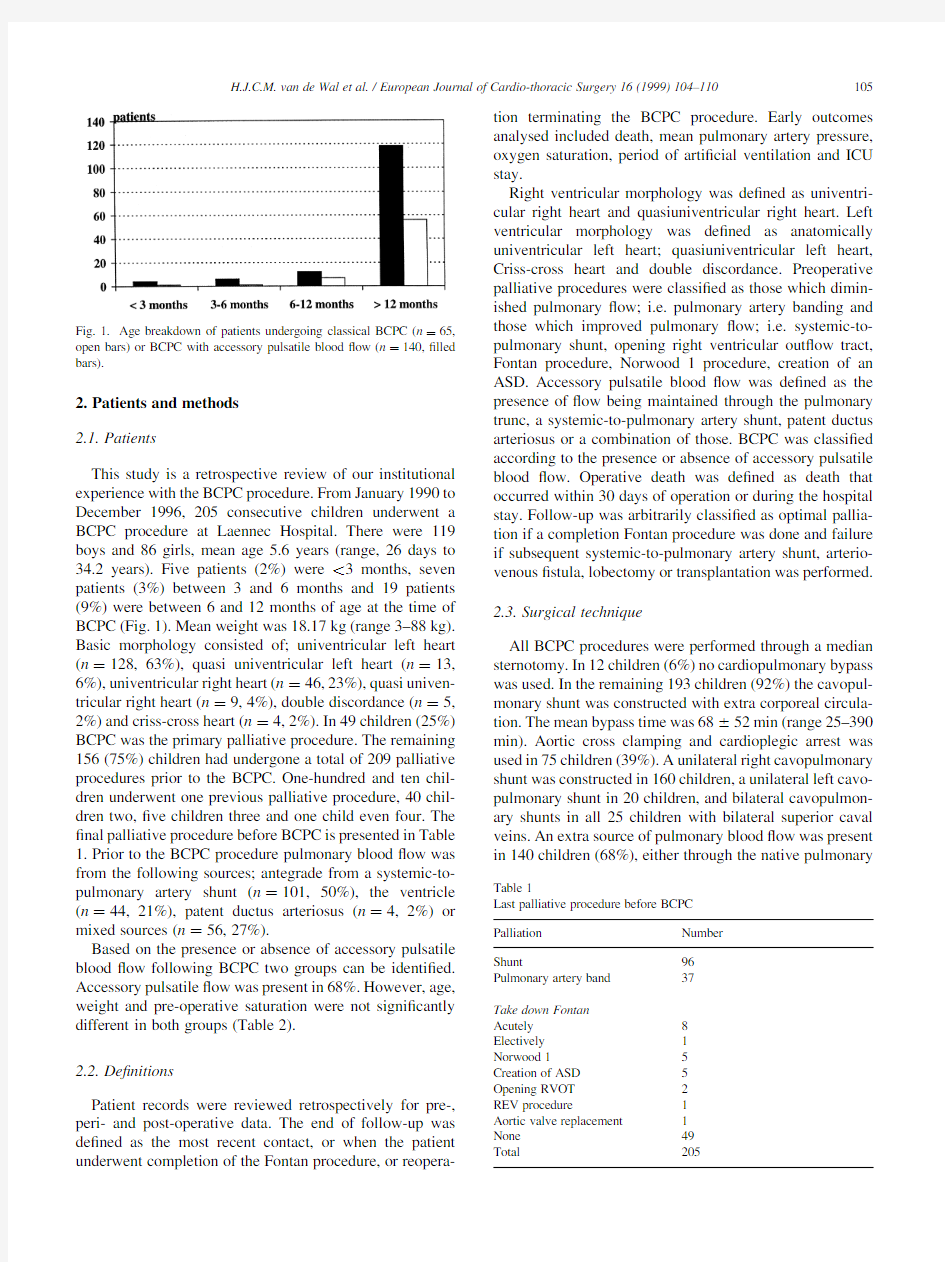
This study is a retrospective review of our institutional experience with the BCPC procedure.From January1990to December1996,205consecutive children underwent a BCPC procedure at Laennec Hospital.There were119 boys and86girls,mean age5.6years(range,26days to 34.2years).Five patients(2%)were,3months,seven patients(3%)between3and6months and19patients (9%)were between6and12months of age at the time of BCPC(Fig.1).Mean weight was18.17kg(range3±88kg). Basic morphology consisted of;univentricular left heart (n 128,63%),quasi univentricular left heart(n 13, 6%),univentricular right heart(n 46,23%),quasi univen-tricular right heart(n 9,4%),double discordance(n 5, 2%)and criss-cross heart(n 4,2%).In49children(25%) BCPC was the primary palliative procedure.The remaining 156(75%)children had undergone a total of209palliative procedures prior to the BCPC.One-hundred and ten chil-dren underwent one previous palliative procedure,40chil-dren two,?ve children three and one child even four.The ?nal palliative procedure before BCPC is presented in Table 1.Prior to the BCPC procedure pulmonary bloodˉow was from the following sources;antegrade from a systemic-to-pulmonary artery shunt(n 101,50%),the ventricle (n 44,21%),patent ductus arteriosus(n 4,2%)or mixed sources(n 56,27%).
Based on the presence or absence of accessory pulsatile bloodˉow following BCPC two groups can be identi?ed. Accessory pulsatileˉow was present in68%.However,age, weight and pre-operative saturation were not signi?cantly different in both groups(Table2).
2.2.De?nitions
Patient records were reviewed retrospectively for pre-, peri-and post-operative data.The end of follow-up was de?ned as the most recent contact,or when the patient underwent completion of the Fontan procedure,or reopera-tion terminating the BCPC procedure.Early outcomes analysed included death,mean pulmonary artery pressure, oxygen saturation,period of arti?cial ventilation and ICU stay.
Right ventricular morphology was de?ned as univentri-cular right heart and quasiuniventricular right heart.Left ventricular morphology was de?ned as anatomically univentricular left heart;quasiuniventricular left heart, Criss-cross heart and double discordance.Preoperative palliative procedures were classi?ed as those which dimin-ished pulmonaryˉow;i.e.pulmonary artery banding and those which improved pulmonaryˉow;i.e.systemic-to-pulmonary shunt,opening right ventricular outˉow tract, Fontan procedure,Norwood1procedure,creation of an ASD.Accessory pulsatile bloodˉow was de?ned as the presence ofˉow being maintained through the pulmonary trunc,a systemic-to-pulmonary artery shunt,patent ductus arteriosus or a combination of those.BCPC was classi?ed according to the presence or absence of accessory pulsatile bloodˉow.Operative death was de?ned as death that occurred within30days of operation or during the hospital stay.Follow-up was arbitrarily classi?ed as optimal pallia-tion if a completion Fontan procedure was done and failure if subsequent systemic-to-pulmonary artery shunt,arterio-venous?stula,lobectomy or transplantation was performed.
2.3.Surgical technique
All BCPC procedures were performed through a median sternotomy.In12children(6%)no cardiopulmonary bypass was used.In the remaining193children(92%)the cavopul-monary shunt was constructed with extra corporeal circula-tion.The mean bypass time was68^52min(range25±390 min).Aortic cross clamping and cardioplegic arrest was used in75children(39%).A unilateral right cavopulmonary shunt was constructed in160children,a unilateral left cavo-pulmonary shunt in20children,and bilateral cavopulmon-ary shunts in all25children with bilateral superior caval veins.An extra source of pulmonary bloodˉow was present in140children(68%),either through the native pulmonary
H.J.C.M.van de Wal et al./European Journal of Cardio-thoracic Surgery16(1999)104±110
105
Fig.1.Age breakdown of patients undergoing classical BCPC(n 65,
open bars)or BCPC with accessory pulsatile bloodˉow(n 140,?lled
bars).
Table1
Last palliative procedure before BCPC
Palliation Number
Shunt96
Pulmonary artery band37
Take down Fontan
Acutely8
Electively1
Norwood15
Creation of ASD5
Opening RVOT2
REV procedure1
Aortic valve replacement1
None49
Total205
artery(n 62),banded pulmonary artery(n 28), systemic-to-pulmonary artery shunt(n 32),pulmonary artery together with a systemic-to-pulmonary shunt (n 14)or patent ductus arteriosus(n 4)(Table3). There was no?xed protocol to treat these patients.The timing as well as type of surgery was based on the individual patient and on the individual surgeon's preference and not on morphological or hemodynamic parameters.Concomi-tant surgical procedures are listed in Table4.
3.Statistical analysis
Data was analysed using a statistical software program (SPSS7.5for Windows).Continuous variables were reported as means and standard deviations(SD)were analysed using unpaired two tailed t-tests.The chi squared statistic,or the Fisher exact where appropriate,was used to determine the signi?cance of the differences between proportions.A value of P,0:05was considered statisti-cally signi?cant.Kaplan±Meier method was used for actuar-ial survival analysis.
4.Results
4.1.Early results
There were eight operative deaths(4%),?ve following BCPC with accessory pulsatile bloodˉow compared to three without accessory pulsatileˉow(not signi?cant). Causes of operative death are presented in Table5. Children with accessory pulsatile bloodˉow had a higher mean pulmonary artery pressure(14.1versus12.6mmHg, P 0:050)and increase of oxygen saturation(12.4%versus 8.7%,P 0:034)at the time of discharge from hospital. The period of post-operative ventilation(1.9days)and length of ICU stay(6days)did not differ in both groups.
https://www.doczj.com/doc/0012788814.html,te results
One-hundred and?fty-three patients were available for
H.J.C.M.van de Wal et al./European Journal of Cardio-thoracic Surgery16(1999)104±110 106
Table2
Patient characteristics
All patients Classical
BCPC BCPC1 accessory ˉow
N20565140
Weight(kg)18.17^15.1816.5^15.418.9^15.1
Age(years) 5.6^6.1 4.7^5.9 5.9^6.1
Saturation at
admission(%)
73^973^874^9
Table3
Additional sources of blood supply before and after cavopulmonary shunt procedure
Native pulmonary
artery anatomyˉow
Last palliation before BCPC Classical BCPC BCPC1accessory
No stenosis57PAB317PA24
Shunt116PA1
PA1shunt3
Shunt1
Norwood152Shunt3
Fontan43PA1
None63PA3
Pulmonary atresia46Shunt4019Shunt20
PDA1
Fontan22±
None41PA1
PDA1
Shunt1
Pulmonary stenosis102Shunt4511PA18
PA1shunt11
Shunt4
PDA1
PAB51PA4
RVOT rec11±
REV11±
Fontan43Shunt1
None465PA38
PDA1
Shunt2 Total20565140
late follow-up,mean follow-up was 2.3years (range 3days to 7.2years).The remaining patients came from abroad and were lost for follow-up.Mean follow up was 1:9^1:6years (range 35days to 7.2years).
During the follow-up period of those children who under-went BCPC with accessory pulsatile blood ˉow (n 95),10underwent completion of the Fontan procedure at a median of 1:7^2:4years.Eight patients underwent reoperation to provide either an extra source of pulmonary blood supply (n 4),arterio-venous ?stula (n 2),heart transplantation (n 1)or lobectomy (n 1).There were four late deaths,due to myocardial failure (n 2),cardio-pulmonary arrest (n 1)and respiratory failure (n 1)(Table 5).
During the period of follow-up of those children who underwent a classical BCPC operation,17children under-went completion of Fontan procedure at a median of 2:7^4:4years after shunting.Fifteen children underwent reoperation either for addition of an extra source of pulmon-ary blood ˉow (n 9),arterio-venous ?stula (n 4),or heart transplantation (n 2).There was one late death due to myocardial https://www.doczj.com/doc/0012788814.html,te mortality between both groups was not signi?cantly different.
The incidence of reoperation following BCPC surgery is not signi?cantly different for both groups.However,if subsequent completion of Fontan is considered the optimal palliation and reoperation to accomplish systemic to pulmonary artery shunt,arteriovenous ?stula and transplan-tation is considered a failure,patients with accessory pulsa-tile ˉow had signi?cantly more and earlier completion of the Fontan procedure (1:7^2:4versus 2:7^4:4years;P 0:008).
Oxygen saturation at last follow-up was signi?cantly higher in children with accessory pulsatile ˉow (mean 85^4%,versus 79^4%;P #0:005).Whereas pre-opera-tive saturation were not different (10:64^9:3for children with accessory pulsatile ˉow versus 6:27^10:0for chil-dren without pulsatile ˉow P 0:016).
Although long term survival is not inˉuenced by age at
BCPC surgery,left or right ventricular morphology or previous systemic to pulmonary artery shunt procedure the survival following BCPC with accessory pulsatile blood ˉow appeared to be signi?cantly better if previous palliative surgery consisted of banding of the main pulmonary artery (P 0:0018).
One child following BCPC with accessory pulsatile blood ˉow developed systemic-to-pulmonary artery collateral's eventually requiring lobectomy.
Actuarial analysis for patients undergoing BCPC with and without accessory pulsatile blood ˉow was not signi?-cantly different,1-,2-and 3-year survival rates following BCPC with accessory pulsatile ˉow 91%,88%and 88%,versus 95%,92%and 92%without accessory pulsatile blood ˉow.During the follow-up interval no further deaths were recorded.5.Discussion
BCPC was initially considered free of the problems asso-ciated with the classical Glenn anastomosis.However,systemic-to-pulmonary arterial collateral's [9],pulmonary arteriovenous ?stulas [10]and systemic venous collateral's [11]have been found to develop more frequently than in other settings of congenital heart disease.The addition of a source of pulsatile ˉow to the pulmonary blood ˉow has been proposed as a potential means of mitigating some of these developments.
The concept of pulsatile cavopulmonary anastomosis was introduced in 1971by Furose [12]in an animal experiment.In 1972Glenn and Fenn [13]recommended creation of an artriovenous ?stula between the axillary artery and vein to augment pulmonary ˉow after a failing cavopulmonary anastomosis.Although the cyanosis was much improved,the patient developed pulmonary hypertension.In 1989Bill-ingsley [14]reported BCPC and accessory pulsatile blood ˉow in the de?nitive biventricular repair of pulmonary atre-sia and intact ventricular septum who had augmentation of
H.J.C.M.van de Wal et al./European Journal of Cardio-thoracic Surgery 16(1999)104±110
107
Table 4
Concomitant surgical procedures
Number
Take down of systemic-to-pulmonary artery shunt
56Ligation of pulmonary trunc 51Pulmonary artery augmentation 35Atrial septectomy
25Closure of atrial septal defect 8Right ventricular outˉow tract reconstruction
4Enlargement of ventricular septal defect
3Damus±Kaye±Stansel procedure 5Atrioventricular valve replacement 1Lung biopsy 7Total
88
Table 5
Causes of death following BCPC procedure
With accessory pulsatile ˉow
Without accessory pulsatile ˉow In hospital or ,30days post-operative Myocardial failure 22Cardiopulmonary arrest ±1Progressive hypoxia 1±Thrombosis of BCPC 1±Mediastinitis 1±Late death
Myocardial failure
21Cardiopulmonary arrest 1±Respiratory failure 1±Total
9
4
the right ventricular outˉow tract and pulmonary artery with a transannular patch.In1991Kobayashi[15]reported the use of BCPC and accessory pulsatile bloodˉow in children who were not suitable for the Fontan procedure.
Well-controlled accessoryˉow to the pulmonary arteries has proven to be an option when a BCPC procedure is performed.Physiologically,there are differences between patients with and without accessory pulsatile bloodˉow, with the quantity of the pulmonaryˉow and the volume load on the ventricle varying in accordance with the amount of additional blood supplied to the pulmonary arteries.The surgeon must be aware of the potential bene?cial inˉuence on pulmonary vascular development and deleterious impact by imposing a volume load on the ventricles[9].If the additional source of pulmonary bloodˉow is not carefully controlled,continued pulmonary recirculation and ventricu-lar dysfunction secondary to a chronic volume overload may result,which has been shown to increase morbidity and mortality after the Fontan operation[16,17].
This study potentially represents one of the largest single institutional studies of patients undergoing BCPC.With rare exceptions[1,5,7,18,19],most reports have comprised fewer than30patients.We have paid particular attention to the inˉuence of accessory pulsatile bloodˉow on the early and medium term results of BCPC.
5.1.Inˉuence of accessory pulsatile bloodˉow on early outcome of BCPC
The main goal of BCPC is to provide perfusion to both lungs while avoiding an excessive increase in systemic venous pressure.One of the factors,which can affect the clinical outcome of the surgically reconstructed circulation, is the amount of pulsatile bloodˉow coming from the main pulmonary artery[9].The hemodynamics in the pulmonary arteries following BCPC with accessory pulsatile bloodˉow can vary from case to case depending on associated problems.Under ideal circumstances,theˉow in the entire pulmonary artery system will be pulsatile.The site of trans-location from venous to arterial pressure in the superior vena cava will depend on the extent of systolic reˉux from the pulmonary artery.The results,however,show that hemodynamics in the pulmonary arteries are greatly inˉuenced by the amount ofˉow through the native main pulmonary artery and that theˉow from the superior vena cava allows an equal distribution of the blood to both lungs, with a small predilection for the left side[20].Non-pulsatile ˉow from BCPC is mainly directed to the ipsilateral lung, whereas pulsatileˉow is directed to the contralateral lung [6].Total perfusion of the ipsilateral lung is less than the perfusion of the contralateral lung[21].In tight pulmonary artery stenosis(.75%),pulsatile forwardˉow is primarily directed to the left pulmonary artery,with little inˉuence on superior vena caval pressure and the right pulmonary artery [22].De Leval[22]also found that pulsatile forwardˉows corresponding to15,30,45and60%of the systemic artery output increased the mean pulmonary artery and superior vena caval pressures by1,1.7,2.4and3.6mmHg,respec-tively.
Despite the two different policies we have demonstrated that accessory pulsatile bloodˉow:
is well tolerated after BCPC and in fact appears to have a small advantage in terms of early post-operative mortal-ity,
mean pulmonary artery pressure and oxygen saturation were signi?cantly higher,
no pulmonary hypertension developed,
appeared not to be a contra-indication for completion of the Fontan procedure.
It is even suggested that if a patient following BCPC has dif?culty in weaning from bypass accessory pulsatileˉow might be bene?cial.
5.2.Chylothorax
Effusions are one of the principal causes of extended hospital stay after BCPC,occurring in approximately10% [23].Frommelt[3]concludes that patients with an addi-tional source of pulmonary bloodˉow after BCPC have a higher postoperative central venous pressure,higher oxygen saturations and are at risk for the late development of a chylothorax.We have been unable to verify this observation in our own cohort.
5.3.Mortality
The reported mortality for BCPC rages from0to33% [1,4,7,15,18,19].Interpretation is complicated by the differ-ent eras of surgery,patient populations and surgical techni-ques.The mortality in the present series(3and5%).
5.4.Inˉuence of accessory pulsatile bloodˉow on late outcome of BCPC
Children with accessory pulsatileˉow showed higher late https://www.doczj.com/doc/0012788814.html,te systemic O2saturation was signi?cantly higher when compared to classical BCPC anastomosis.If subsequent Fontan procedure is the optimal palliation and a systemic-to-pulmonary artery shunt,arterio-venous?stula or transplantation is considered as failure,patients with accessory pulsatileˉow have a higher rate at an earlier age of completion Fontan procedure.The Fontan procedure was not performed electively,despite the fact that in the group of BCPC with accessory pulsatile bloodˉow, pulmonary vascular resistance might have become too high.The criteria to proceed with a Fontan procedure were:decreasing exercise capacity or increasing cyanosis due to insuf?cient pulmonaryˉow,with low pulmonary vascular resistance.
Previous reports[6,7,15]have focused on the hemody-namic and clinical effects of BCPC associated with acces-sory pulsatileˉow.Muster[6]demonstrated that BCPC may
H.J.C.M.van de Wal et al./European Journal of Cardio-thoracic Surgery16(1999)104±110 108
be successfully used to accomplish the so-called`one and one-half repair'.Kobayashi[15]described10high risk Fontan candidates who underwent BCPC with accessory pulsatileˉow.Webber[7]in a multi-institutional study described108patients and concluded that accessory pulsa-tileˉow is well tolerated in the short and medium term and that early post-operative saturation improved.
Our data show that long term survival following BCPC with accessory pulsatileˉow is signi?cantly better if previous palliative surgery had included banding of the main pulmonary artery.Although Reddy[5]reported age less than2months at time of BCPC as a signi?cant predictor of poorer survival.We have been unable to verify the other observations in other reports.
5.5.Consequences for the pulmonary circulation
The haemodynamic consequences of BCPC on the pulmonary circulation are less well understood.Several authors have drawn attention to the potential bene?ts of leaving pulsatileˉow in the pulmonary arteries after BCPC[6,8,15].Kobayashi[15]emphasised the possible bene?cial effects of accessory pulsatileˉow in preventing late development of pulmonary arterio-venous malforma-tions.
Although there are many reports of arteriovenous malfor-mations after classical Glenn shunt[24,25],there are only two reported cases of pulmonary arteriovenous malforma-tions after the Fontan operation[26].Possible causes of pulmonary arteriovenous malformations after Glenn proce-dures;
time:the Glenn shunt has been used for more than30 years,whereas the Fontan operation has been widely applied for only the past10years.
`hepatic factor':perhaps the absence of some important interaction between a hepatic factor and lung blood vessels induces formation of arteriovenous malformations after the Fontan operation.
If a`hepatic factor'[8]is important for the prevention of pulmonary arteriovenous malformations this might repre-sent an advantage of BCPC with accessory pulsatileˉow. However in one of our patients with BCPC with accessory pulsatileˉow pulmonary arteriovenous malformations developed,necessitating lobectomy.To our knowledge we are the?rst to report this complication following BCPC with accessory pulsatileˉow.In addition pulmonary bloodˉow has been advocated as a means of promoting pulmonary arterial growth.There are few published data to support or disapprove these assumptions[10].
6.Conclusions
Although,there now seems to be consensus that pulsati-lity is not useful to improve the operative mortality of the Fontan operation and there is widespread speculation that absence of pulsatility may contribute to the late deleterious effects of this procedure.Our data suggest that BCPC with accessory pulsatileˉow compared to classical BCPC can: be safely performed;
gives at late follow-up higher oxygen saturation's; does not develop pulmonary hypertension cq is no contra-indication for Fontan
have more and earlier completion of Fontan procedure. Acknowledgements
The authors would like to thank Steven Chamuleau for his assistance with the statistical analysis and Stephen R. Woolley FRCS for his help in preparing the manuscript.
References
[1]Bridges,N.D.,Jonas,R.A.,Mayer,J.E.,Flanagan,M.F.,Keane,J.F.,
Castaneda,A.R.Bidirectional cavopulmonary anastomosis as interim palliation for high risk Fontan candidates:early results.Circulation 1990;82(suppl IV):IV170-IV176.
[2]Castaneda AR.From Glenn to Fontan:a continuing evolution.Circu-
lation1992;86(suppl.II):II80±II84.
[3]Frommelt MA,Frommelt PC,Berger S,Pelech AN,Lewis DA,
Tweddell JS,Litwin SB.Does an additional source of pulmonary bloodˉow alter outcome after a bidirectional cavopulmonary shunt?Circulation1995;92(suppl.II):II240±II244.
[4]Chang AC,Hanley FL,Wernovsky G,Rosenfeld HM,Wessel DL,
Jonas RA,Mayer JE,Lock JE,Castaneda AR.Early bidirectional cavopulmonary shunt in young infants.Circulation1993;88:149±158.
[5]Reddy VM,McElhinney DB.Moore,Ph.Bristow,J.,Haas,G.S.,
Hanley,F.L.An institutional experience with the bidirectional cavo-pulmonary shunt:do we know enough about it?Cardiol Young 1997;7:284±293.
[6]Muster AJ,Zales VR,Ilbawi MN,Backer CL,Duffy CE,Mavroudis
C.Biventricular repair of hypoplastic right ventricle assisted by pulsa-
tile bidirectional cavopulmonary anastomosis.J Thorac Cardiovasc Surg1993;105:112±119.
[7]Webber SA,Horvath P,LeBlanc JG,Slavik Z,Lamb RK,Monro JL,
Reich O,Hruda J,Sandor GGS,Keeton BR,Salmon AP.Inˉuence of competitive pulmonary bloodˉow on the bidirectional superior cavopulmonary shunt:a multi-institutional study.Circulation 1995;92(suppl.II):II279±II286.
[8]Jonas RA.The importance of pulsatileˉow when systemic venous
return is connected directly to the pulmonary arteries.J Thorac Cardi-ovasc Surg1993;105:173±188.
[9]Triedman JK,Bridges ND,Mayer JE,Lock JE.Prevalence and risk
factors for aortopulmonary collateral vessels after Fontan and bidir-ectional Glen procedures.J Am Coll Cardiol1993;22:207±215. [10]Bernstein HS,Brook MM,Silverman NH,Bristow J.Development of
pulmonary arteriovenous?stulae in children after cavopulmonary shunt.Circulation1995;92(suppl.II):II309±II314.
[11]Gatzoulis MA,Shinebourne EA,Redington AN,Rigby ML,Ho SY,
Shore DF.Increasing cyanosis early after cavopulmonary connection caused by abnormal systemic venous channels.Br Heart J 1995;73:182±186.
[12]Furose A,Brawley RK,Gott VL.Pulsatile cavopulmonary artery
shunt.J Thorac Cardiovasc Surg1972;63:459±500.
[13]Glenn WWL,Fenn JE.Axillary arteriovenous?stula.A means of
supplementing bloodˉow through a cava-pulmonary artery shunt.
Circulation1972;46:1013±1017.
[14]Billingsley AM,Laks H,Boyce JW,George B,Santulli T,Williams
H.J.C.M.van de Wal et al./European Journal of Cardio-thoracic Surgery16(1999)104±110109
RG.De?nitive repair in patients with pulmonary atresia and intact ventricular septum.J Thorac Cardiovasc Surg1989;97:746±754. [15]Kobayashi J,Matsuda H,Nakano S,Shimazaki Y,Ikawa S,Mitsuno
M,Takahashi Y,Kawashima Y,Arisawa J,Matsushita T.Hemody-namic effects of bidirectional cavopulmonary shunt with pulsatile pulmonaryˉow.Circulation1991;(suppl III):III219±III225. [16]Graham TP,Franklin RCG,Wyse RKH,Gooch V,Dean?led JE.Left
ventricular wall stress and contractile function in childhood:normal values and comparison of Fontan versus palliation only in patients with tricuspid atresia.Circulation1986;74(suppl.I):I61±I69. [17]Sluysmans T,Saunders SP,van der Velde M,Matitiau A,Parness IA,
Spevak PJ,Mayer JE,Colan SD.Natural history and patterns of recovery of contractile function in single ventricle after Fontan opera-tion.Circulation1992;86:1753±1761.
[18]Hawkins JA,Shaddy RE,Day RW,Sturtevant JE,Orsmond GS,
McGough EC.Mid term results after bidirectional cavopulmonary shunts.Ann Thorac Surg1993;56:833±837.
[19]Pridjian AK,Mendelsohn AM,Lupinetti FM,Beekman RH,Dirk M,
Serwer G,Bove https://www.doczj.com/doc/0012788814.html,efulness of the bidirectional Glen procedure as staged reconstruction for the functional single ventricle.Am J Cardiol 1993;71:959±962.
[20]Migliavacca F,de Leval MR,Dubini G,Pietrabissa R.A computa-
tional pulsatile model of the bidirectional cavopulmonary anastomo-sis:the inˉuence of pulmonary forwardˉow.J Biomech Eng 1996;118:520±528.
[21]Reich O,Horvath P,Ruth C,Krejcir M,Skovranek J.Pulmonary
blood supply in bidirectional cavopulmonary anastomosis with pulsa-tile pulmonary bloodˉow:quantitative analysis using radionuclide angiocardiography.Heart1996;75:513±517.
[22]de Leval MR,Dubini G,Migliavacca F,Jalali H,Camporini G,
Redington A,Pietrabissa https://www.doczj.com/doc/0012788814.html,e of computationalˉuid dynamics in the design of surgical procedures:application to the study of compe-titiveˉows in cavo-pulmonary connections.J Thorac Cardiovasc Surg1996;111:502±513.
[23]Mainwaring RD,Lamberti JJ,Uzark K,Spicer RL.Bidirectional
Glenn:is accessory pulmonary bloodˉow good or bad?Circulation 1995;92(suppl II):II294±II297.
[24]Kopf GS,Laks H,Stansel HC,Hellenbrand WE,Kleinman CS,
Talner NS.Thirty year follow-up of superior vena cava-pulmonary artery(Glenn)shunts.J Thorac Cardiovasc Surg1990;100:662±671.
[25]Trusler GA,Williams WG,Cohen AJ,Rabinovitch M,Moes F,
Smallhorn JF,Coles JG,Lightfoot NE,Freedom RM.The cavopul-monary shunt:evaluation of a concept.Circulation1990;82(suppl IV):IV131±IV138.
[26]Moore JW,Kirby WC,Madden WA,Gaither NS.Development of
pulmonary arteriovenous malformations after modi?ed Fontan opera-tions.J Thorac Cardiovasc Surg1989;89:1045±1050.
Appendix A.Conference discussion
Dr J.A.van Son(Leipzig,Germany):In our experience and that of others bi-directional cavopulmonary anastomosis with an additional source of pulmonary bloodˉow has a higher post-operative morbidity rate than bi-directional cavopulmonary anastomosis without accessory bloodˉow.In the majority of your patients the cavopulmonary anastomosis was performed beyond1year of age,which I think is rather late in terms of avoidance of volume overloading of the single ventricle and its related detrimental sequelae.Please comment on the concept of performing the bi-directional cavopulmonary anastomosis before6months of age.
Dr van de Wal:We have not been able to show in our retrospective analysis that age is a signi?cant factor,indeed although theoretically the presence of an accessory pulmonary bloodˉow might increase the potential for volume overload,in practice our experience does not con?rm this.As regards the possibility of performing the bi-directional cavopulmonary anastomosis before6months of age I think we should be guided by the experience in other congenital defects where clearly as our own expertise increases so the age of de?nitive operation tends to decrease.
Dr S.Conte(Leuven,Belgium):You used bi-directional Glenn and accessoryˉow both as intermediate stage to Fontan and as end-stage alter-native to Fontan.Assuming from the data that you presented that this procedure is better than bi-directional Glenn alone as an end-stage,do you have comparative hemodynamic or clinical data in patients after Fontan completion to support bi-directional Glenn and accessoryˉow also as intermediate stage?And did you never have to renounce to Fontan comple-tion because of the accessoryˉow?
Dr van de Wal:No.The Fontan operation was the end-stage of measurement.So we followed up those patients who had a bi-directional Glenn,with or without accessoryˉow,and measured the period until last clinic follow-up or death or completion of Fontan operation,as the end point for this study,therefore,I can't answer the question of what happened after their Fontan operation.
Dr S.Conte:And did you have to renounce Fontan completion because of the accessoryˉow in any patient?
Dr van de Wal:No.
Dr H.Jalali(Queensland,Australia):I studied similar patients like yours,and we had140patients with bi-directional Glenn and maintenance of some forwardˉow.The results were presented last year in Sydney,with very similar conclusions to yours in regard to better oxygenation and not compromising the long term.But there were12patients out of140,which is nearly10%,which failed at the time of the primary operation.And what I call failure was things such as highly elevated and pulsatile central venous pressure beyond20±25.Did you have any of these early failures in your experience?
Dr van de Wal:We have not been able to show in our retrospective analysis that age is a signi?cant factor,indeed although theoretically the presence of an accessory pulmonary bloodˉow might increase the potential for volume overload,in practice our experience does not con?rm this.As regards the possibility of performing the bidirectional cavopulmonary anastomosis before6months of age I think we should be guided by the experience in other congenital defects where clearly as our own expertise increases so the age of de?nitive operation tends to decrease.
Dr Jalali:But you didn't take anyone back to suppress the accessory ˉow?
Dr van de Wal:Not that I am aware of,no.
H.J.C.M.van de Wal et al./European Journal of Cardio-thoracic Surgery16(1999)104±110 110
浅谈桥梁下部结构的选型及施工设计便于后期养护 李红军 (哈密公路总段,新疆哈密 839000) 摘要:在桥梁设计的过程中,下部结构的考虑是否得当,对工程造价、工程质量及后期养护使用影响很大,本文结合我在近几年一些施工设计项目有关资料的基础上,对桥梁墩、台的形式选择及结构设计注意事项进行了初步探讨。 关键词:桥梁下部;结构选型;设计与计算;经济 1 桥台结构型式选用 1.1 底部设有支撑梁的轻型桥台 轻型桥台的特点是,台身体积较小,台身为直立的薄壁墙,台身两侧设有翼墙(用于挡土),可以将侧墙做成斜坡。在两桥台下部设置钢筋混凝土支撑梁,上部结构与桥台通过锚栓连接,构成四铰框架结构系统,并借助两端台后的土压力来保持稳定。这种桥台适用于小跨径桥梁,桥跨孔数与轻型桥墩配合使用时不宜超过三孔,且桥梁全长不宜大于20m,单孔跨径不宜大于13m。按照翼墙(侧墙)的形式和布置方式,这种桥台又可分为:一字形轻型桥台、八字形轻型桥台、耳墙式轻型桥台。 1.2 钢筋混凝土薄壁桥台 薄壁轻型桥台常用的形式有悬臂式、扶壁式、撑墙式、及箱式等。这种桥台是由带扶壁的前墙和侧墙以及水平底板构成。挡土墙由前墙和间距为2.5~3.5m的扶壁组成。台顶由竖直小墙和支于扶壁上的水平板构成,用于支承桥跨结构。两侧薄壁可以与前墙垂直,有时也做成与前墙斜交。相对于重力式桥台而言,可减少污工体积40%~50%,同时因自重减轻而减少了对地基的压力,适用于软土地基的条件,但其构造和施工均较复杂,且用钢量较多。当墩台填土不高,河床不宽时,为了减少桥长,降低造价,不让台前溜坡压缩河床,可采用靠河较近墩台身直立的桩基础薄壁墩台,墩台下面设置支撑梁,整个桥梁形成框架结构体系,并借助两端台后的被动土压力来保持稳定。从已建成通车的公路上的桥梁(下部结构多采用这种型式)来看,情况良好。 1.3 埋置式桥台 埋置式桥台是将台身埋在锥形护坡中,这样,桥台所受的土压力大为减小,桥台的体积也就得到相应减小。但是由于台前护坡是用片石(或混凝土)作表面防护的一种永久性设施,存在着被洪水冲毁而使台身裸露的可能,故设计时必须进行强度和稳定性验算。按台身的结构形式,埋置式桥台可以分为:肋形埋置式桥台、桩柱式埋置式桥台、和框架式桥台。肋形埋置式桥台的台身是由两块(或多块)后倾式的肋板与顶面帽梁连接而成。台高在10m及10m以上者须设置横向系梁。帽梁、系梁和耳墙均需配置钢筋。桩
思想作风整顿查摆问题个人剖析材 料三篇 篇一:解放思想个人剖析及自查整改材料 自开展解放思想活动以来,我自身能够按照局党组活动实施方案的安排,积极参与到这次活动中,并在认真学习的同时,围绕思想作风整顿的具体内容,对照自己平时的实际工作及思想动态,认真查摆了在思想作风、工作态度等方面存在的问题,并对其进行了深层次的剖析,以期达到自我教育、自我提高、自我完善目的。 一、主要问题 自参加工作以来,在领导和同志们的帮助下,虽然做了一些工作,较为认真地完成了领导交办、本职范围内的工作,但是对照解放思想查摆问题阶段的实施方案还存在不少问题,在思想政治素质方面还不能完全适应新形势、新任务的要求,主要有以下几个方面: 一是理论学习不主动,自觉性不高。不能自觉主动抽时间静下心来学习,利用工作空闲和业余时间学习也比较少。经常是上级要求学什么就学什么,与工作关系密切的多学,与工作关系不大的少学,常常是需要什么学什么,急用什么学什么,碰到材料才找依据、查资料。没有系统地学习一些现代法律知识和环保知识,特别是对政治理论的学习重视程度不够,不能够深刻理解和领会社会主义法治理念的实质内涵,对于利用社会主义法治理念全面指导自己的工作和学习的重要性还缺乏必要的认识。 二是业务功底不够扎实,虽然对工作有所了解,但也只是只知皮毛,掌握知识
不全,尤其是对一些其它部门专业知识知之甚少,由于自身综合素质不高,缺 乏对全局性的把握,不能很好地理解领导意图。虽然自己目前工作积极,但也 还颇感吃力,连自己都不是很满意,业务素质亟待提高。 三是工作被动落实多,主动超前少。大多是承办领导交办事项,工作中经常是 处于奉命行事,落实任务,不能做到想领导之未想,超前思考、提前预测、及 时准备;谋领导之所谋,深入调研,提供资料、当好参谋。对工作往往是兵来 将挡,水来土掩,疲于应付。工作的全局性、前瞻性、创新性不够,为领导服 务少,与领导要求有相当差距。 二、存在问题的原因经过剖析,自己感到存在这些问题的原因是多方面的 一是思想观念比较陈旧。由于未能做到系统研读原著,在其精神实质的掌握上 又不求甚解,思想理论素质未能得到有效提高。因而不善于用理论指导实践, 在工作中很难有所创新,在理论学习中,没有很好地坚持理论联系实际,没能 及时用科学思想分析出现问题的原由,及时纠正主观认识上出现的偏差。同时 认为有一定的基础,足可以应付目前的工作,对更新知识的紧迫性和必要性缺 乏深刻的认识。二是认识上存在偏差。工作上不求有功,但求无过,不求过得硬,但求过得去,缺乏积极进取的精神,满足于完成领导交办的工作任务,对 如何开拓性地开展工作研究不够,有时甚至流露出马马虎虎,得过且过的思想,工作缺乏主动性和积极性。对自己所从事工作的重要性认识不够,体会不深, 总感到从事工作太辛苦,从而导致有推、拖、等的思想,降低了自己的工作标 准和要求。事实上,在新形势下,工作涉及面广,作为一名工作人员,要学习 的知识很多,如何为领导当好参谋助手,提供决策的依据,是很值得深入探讨 和研究的问题。
建筑结构模型设计中的选型与设计 高层建筑的结构体系是高层结构是否合理、经济的关键,随着建筑高度和功能的发展需要而不断发展变化。论文总结了各种高层建筑结构体系、特别是近年来出现的复杂、新颖的结构体系的受力特征,进而对高层建筑结构选型要点进行了探讨。 标签:建筑结构;模型设计;选型与设计 一、结构选型 (一)框架结构体系 框架结构体系采用梁、柱组成的结构体系作为建筑竖向承重结构,并同时承受水平荷载,适用于多层或高度不大的高层建筑。框架结构的布置要注意对称均匀和传力途径直接。传统的结构布置采用主次梁的作法为主,逐步向扁梁或无盖梁发展。框架柱是框架结构的主要竖向承重和抗侧力构件,以受压应力为主。 (二)剪力墙结构体系 剪力墙结构体系是利用建筑物的墙体作为竖向承重和抵抗侧力的结构体系。剪力墙的间距受楼板构件跨度的限制,一般为3~8米。因而剪力墙结构适用于要求小房间的住宅、旅馆等建筑。 (三)框架一剪力墙结构体系 框架一剪力墙结构是将框架和剪力墙结合在一起而形成的结构形式。它既有框架结构平面布局灵活、适用性强的优点,又有较好的承受水平荷载的能力,是高层建筑中应用比较广泛的一种结构形式。合理的结构设计,将能使框架、剪力墙两种不同变形性能的抗侧力结构很好地协同工作,共同发挥作用。 (四)筒体结构 随着建筑物高度的增加,传统的框架结构体系、框架一剪力墙结构体系已不能很好地满足结构在水平荷载作用下强度和刚度的要求。筒体体系因其在抵抗水平力方面具有良好的刚度,并能形成较大的使用空间,而成为六十年代以后常用于超高层建筑中的一种新的结构体系。根据筒体布置、组成、数量的不同,又可分为框架筒体、筒中筒、组合筒三种体系。 二、结构设计 (一)地基与基础设计
结构选型与布置第一节结构设计知识要点 优秀的建筑设计应做到艺术、技术和经济性的三位一体,它是建筑师对这三方面知识充分掌握和创造性应用的产物。建筑师在完成建筑功能、建筑艺术性设计的同时,也应当兼顾建筑的安全性、适用性、耐久性和经济性,以便建筑设计时其他工种的同事能同自己良好的衔接。 在建筑技术设计作图中,首先要根据建筑平面布置及房屋层数和高度,选用合理的结构体系,如:砌体结构、框架结构、剪力墙结构、框架-剪力墙结构等。其次要合理地确定和布置竖向承重构件和抗侧力构件,这些构件一般包括:承重墙体、柱、框架和支撑等。墙体既是竖向承重构件,又是抗侧力构件,同时又是建筑平面分隔和围护的需要;框架是由梁和柱刚性连接组成的骨架,它能承受建筑物的竖向荷载,同时也能承担水平荷载(如风力、地震作用) ;支撑是作为承担建筑物水平荷载的专用构件,主要用于单层产房、钢结构和高层建筑中。再次是合理地选择楼(屋)盖体系,楼(屋)盖体系构件包括:楼板(屋面板)、梁系(屋架)。楼板主要功能是沿水平方向分隔建筑中的上下空间,将其承受的建筑使用荷载传递给梁系或直接传给框架梁;使用梁系主要是为了使较大空间的房间传力途径更加合理,梁系中次梁将荷载传递给主梁或框架梁,再传至柱或墙。最后应合理地选择基础形式,根据不同的结构体系、建筑体型和场地土类别为竖向承重构件选取合理的基础形式,例如带拉梁或不带拉梁的独立基础、条形基础、箱形基础、役形基础、桩基础等。 下面将主要介绍砌体结构、框架结构、剪力墙结构和框架-剪力墙结构的结构布置注意事项。 一、砌体结构 砌体结构有着悠久的历史和辉煌的记录,直至今日仍然广泛地应用在各类工业与民用建筑中。砌体结构有造价低廉、易于取材、建筑舒适度好、建筑能耗低、耐久性好、维护方便、抗火性能优异、施工设备和方法简单、外观优美等优势;同样也存在着强度低、材料用量多、自重大、砌筑质量较难保证、震害严重等问题。 (一)砌体结构的承重墙体系 1.横墙承重体系 横墙指横向承重墙体。横墙承重体系指建筑物楼(屋)盖的竖向荷载主要通过短向楼板或横墙间小梁传给横墙,再经横墙基础传至地基的结构体系。由于横墙是主要承重墙体, 它的间距不能太大,划分房屋开间的宽度一般为3~5m,即横墙间距。横墙承受两侧开间内由楼(屋)盖传来的竖向荷载和由风或横向水平地震作用产生的水平荷载,假若两侧开间宽度相同,横墙在竖向荷载作用下基本上处于轴心受压状态,在水平荷载作用下则处于受弯、受剪状态。横墙承重体系建筑物的纵墙不参与承受楼(屋)盖荷载,仅承受自身的重量,因而在纵墙上可开设较大的门窗洞口;又由于承重横墙较密,建筑物的整体刚性和抗震性能很好,这些都是又由于横墙较密而使建筑材;内空间较小室,这种体系在房间使用上很不灵活,横墙承重体系的优点。但是 料用量较大,这又是横墙承重体系的缺点。横墙承重体系适用于宿舍、住宅等建筑物。 2.纵墙承重体系 纵墙指纵向承重墙体。纵墙承重体系指建筑物楼(屋)盖的竖向荷载主要通过长向楼板或进深梁传给纵墙,再经纵墙基础传至地基的结构体系。在这个体系中,为了保证建筑物的整体刚性,沿纵墙方向一定长度还需设置少量横墙与纵墙拉结。这样,建筑物的竖向荷载基本上由纵墙承受,而由风或横向水平地震作用产生的水平荷载则主要通过水平楼(屋)再传给横墙。由于板、梁在纵墙上的支承点往往并不与纵墙形心线重合,故纵墙一般处于偏心受压状态,而横墙在水平荷载作用下则处于受剪和受弯状态。纵墙承重体系的横墙间距一般较大,使得建筑物可以有较大的房间,室内分割也较灵活,这是它的优点;但整个建筑物的整体刚性不如横向承重体系,在纵墙上开门窗洞口受到限制,这又是它的缺点。纵墙承重体系适用于教学楼、办公楼、实验室、阅览室、中
建筑结构选型结课论文悬索结构的形式和设计选型 姓名:李超 学号:1401102-01 所在院系:建筑与城市规划学院 学科专业:城乡规划 指导教师:张弘 二〇一六年十二月
标题:悬索结构的形式和设计选型 申明:本人申明提交作业文章所有内容均有本人完成,文中引用他人观点均已标明出处。 签字: 日期:
悬索结构的形式和设计选型 摘要:本文在简述悬索结构构成和受力特点的基础上,根据索网曲面形式和结构特征,何恳索结构迸仃了分类,介绍了各种单(双)曲面单(双)层悬索结构、交叉索网、斜拉结构的组成特点和国内外卜程应用状况。文章还对悬索结构设计选型的若干主要问题,如建筑平面形状、结构跨度、刚度与稳定性、边缘构件与支承结构、片画材料与排水等进行了论述,并提供了一些可供设计参考的有效措施。 关键词:悬索结构设计选型索网杂交结构 1.悬索结构的组成与发展 土木建筑结构所指的悬索结构,就是指以柔性拉索或将拉索按一定规律布置成索网来直接承受屋面荷载作用的结构(见图1)这些索或索网均悬挂在支承结构体系的边缘构件上。在竖向荷载作用下,索或索网均承受轴向拉力,并通过边缘构件和支承结构将这些拉力传递到建筑物的基础上去。 悬索结构中承受轴向拉力的柔性拉索多采用高强度钢丝组成的钢铰线、钢丝绳、钢丝束等,有的也可以采用圆钢筋或带状薄钢板。边缘构件是用来锚固拉索(索网)的,起到承受索在支座处的拉力作用。根据建筑平面和结构类型的不同,
边缘构件可以选用圈梁、拱、析架、刚架等劲性构件,也可以直接选用柔性拉索。支承结构主要是用作承受边缘构件传来的压力和水平推力引起的弯矩。常选用钢筋混凝土独立柱、框架、拱等结构形式。这样受拉的索网和以受压、受弯为主 的边缘构件和支承结构,就可以分别采用受拉强度较高的钢材和抗压强度较好的钢筋混凝土,使不同材料的力学性能能得到合理利用。由于对柔性拉索与刚性结构的优化组合,就可以用较少的材料(一般索的用钢量仅为普通钢结构的l/5一 1/7,11一般都在10kg/m以下)做成较大跨度的悬索结构。由于钢索自重很轻,屋面构件也不很大,囚而给施工架设带来了很大的方便。安装时不需大型起重设备,也不需另设脚手架。这些都有利于加快施工进度,降低工程造价。同时索网布置灵活,便于建筑造型,能适应平面形状与外形轮廓的各种变化,这使建筑与 结构可以得到较完美的结合。因此悬索结构在友跨度建筑中得到了越来越多的应用。 悬索结构是一种受力比较合理的建筑结构形式。它与简支梁受力情况对比,就可以看出这种合理性。众所周知,图2中的简支梁住竖向荷载作用下,上纤维压应力的合力与「纤维拉应力的合力组成了截面的内力矩.合力间的距离即为内力臂,它总在截面高度的范围内,因此要提高梁的承载能力,就意味着要增加梁的高度。但在悬索结构中,钢索在自重下就自然形成了垂度,由索中拉力与支承水平力间的距离构成的内力臂,总在钢索截面范围以外,增加垂度也就加大了力臂,从而可以有效地减少索中拉力和钢索截面面积。
关于高层建筑结构选型设计的初步探讨【摘要】:高层建筑的结构体系是高层结构是否合理、经济的关键,随着建筑高度和功能的发展需要而不断发展变化。论文总结了各种高层建筑结构体系、特别是近年来出现的复杂、新颖的结构体系的受力特征,进而对高层建筑结构选型要点进行了探讨。 【关键词】:高层建筑;结构选型;重要性; 中图分类号: tu97 文献标识码:a 文章编号: 【 abstract 】:the structure of the high-rise building system is high-rise structure whether reasonable, key economic, along with the development of building height and function need constantly develops and changes. the thesis summed up the various kinds of high building structure system, especially in recent years, the complex, novel appeared of structural system of the mechanical characteristics and structure design of high-rise building points are discussed 【 key words 】: high-rise buildings; the structural type; importance; 引言 对于高层建筑的结构设计, 首先摆在结构工程师面前的是结构选型的问题。高层建筑结构的选型通常要遵循一定的原则, 它不仅考虑到建筑物的适用性、经济性、抗震性能,而且要考虑施工安装的影响。正确处理高层建筑结构体系的选型问题,对于高层建筑结
手机音腔部品选型及音腔结构设计指导及规范 Company Document number:WTUT-WT88Y-W8BBGB-BWYTT-19998
手机音腔部品选型及音腔结构设计指导及规范 1. 声音的主观评价 声音的评价分为主观和客观两个方面,客观评价主要依赖于频响曲线﹑SPL值等声学物理参数,主观则因人而异。一般来说,高频是色彩,高中频是亮度,中低频是力度,低频是基础。音质评价术语和其声学特性的关系如下表示: 从人耳的听觉特性来讲,低频是基础音,如果低频音的声压值太低,会显得音色单纯,缺乏力度,这部分对听觉的影响很大。对于中频段而言,由于频带较宽,又是人耳听觉最灵敏的区域,适当提升,有利于增强放音的临场感,有利于提高清晰度和层次感。而高于 8KHz略有提升,可使高频段的音色显得生动活泼些。一般情况下,手机发声音质的好坏可以用其频响曲线来判定,好的频响曲线会使人感觉良好。 声音失真对听觉会产生一定的影响,其程度取决于失真的大小。对于输入的一个单一频率的正弦电信号,输出声信号中谐波分量的总和与基波分量的比值称为总谐波失真(THD),其对听觉的影响程度如下:THD<1%时,不论什么节目信号都可以认为是满意的; THD>3%时,人耳已可感知; THD>5%时,会有轻微的噪声感; THD>10%时,噪声已基本不可忍受。 对于手机而言,由于受到外形和Speaker尺寸的限制,不可能将它与音响相比,因此手机铃声主要关注声音大小、是否有杂音、是否有良好的中低音效果。 2. 手机铃声的影响因素 铃声的优劣主要取决于铃声的大小、所表现出的频带宽度(特别是低频效果)和其失真度大小。对手机而言,Speaker、手机声腔、音频电路和MIDI选曲是四个关键因素,它们本身的特性和相互间的配合决定了铃声的音质。 Speaker单体的品质对于铃声的各个方面影响都很大。其灵敏度对于声音的大小,其低频性能对于铃声的低音效果,其失真度大小对于铃声是否有杂音都是极为关键的。
护岸结构选型和设计分析 发表时间:2019-06-18T16:22:18.140Z 来源:《防护工程》2019年第5期作者:王创江 [导读] 河道生态治理是生态建设的重要环节,生态护岸形式和材料的选取应结合当地特色,就地取材,因地制宜,合理规划。陕西省土地工程建设集团陕西西安 710075 摘要:根据地形、水文、地质等资料分析现状及存在的问题,结合结构和景观需求,分析常用护岸的优点和缺点,通过方案比选,左岸护坡材料选用格宾石笼护坡,右岸护坡材料选用混凝土栽植槽护岸。设计确定结构形式和尺寸,结果表明:结构满足在设计洪水位和施工期两种工况下临水侧堤坡的稳定性。 关键词:格宾石笼护坡混凝土栽植槽稳定性 中图分类号:TV871.1;文献标识码:A 河道部分河段有堤岸,原有堤岸防洪标准较低;两岸道路兼做堤岸,没有完善的防洪体系;河道两岸坡地杂草丛生,沿河高度2m~10m,天然状态下稳定性良好,现状河堤抗冲能力差,水土流失严重,生态环境差,存在安全隐患。根据水流作用、地质地貌、施工环境等因素,选定适宜本工程的护岸型式是保证堤防和防洪的重要保证措施。 1常用护岸形式选择 从防冲刷、亲水、生态、造价、美观等方面考虑,拟选用生态混凝土、格宾石笼、预制连锁块、植生型雷诺护垫、混凝土栽植槽五种护坡材料进行比较。 1.1生态混凝土护坡 生态混凝土是一种能将工程防护和生态修复很好的结合起来的新型护坡材料,性能介于普通混凝土和耕植土之间的新型材料[1],具有一定的强度,质量相对较小,自重轻,形成一个个“蜂窝状”空隙,既有利于植被根系生长,又能为植被生长所必需的养分提供存储空间[2]。生态混凝土护岸具有抗冲能力强、施工速度快、生态效果好等优点。 2)格宾石笼护坡 格宾石笼护岸具有很好的柔韧性、透水性,对于不均匀沉降自我调整性能佳,耐久性强,操作简单、施工速度快,受气候影响较小,适用于机械化施工,大大缩短了工期。同时,因岸面多孔性,石材间有利于动植物生长,较好的实现了工程结构和生态环境的有机结合,但是格宾石笼对块石料需求量和强度要求高。 3)预制块联锁式护岸 预制块联锁式护岸由拼装和整体两部分组成,护坡厚度较薄,具有灵活性好、透水性好、生态效果好等优点,但是联锁式护岸施工工艺要求较高,易因堤身的不均匀沉降而开裂,一般适应于流速小于3m/s的河道,且产品的安装质量控制难度大。 4)植生型雷诺护垫 植生型雷诺护垫由雷诺护垫底座和加筋麦克垫盖板组成,整体性好,综合了纯刚性与纯柔性结构的特点,有较强的的河床变形适应能力,有效的解决了不均匀沉降问题,施工便利,还具备促淤特性,能更有效的抵抗水流作用和促进植被生长,稳固边坡。 5)混凝土栽植槽护岸 混凝土栽植槽护岸的核心材料为自嵌块。这种护坡型式是一种重力结构,主要依靠自嵌块块体的自重来抵抗动静荷载,使岸坡稳固;同时该种挡土墙无需砂浆砌筑,主要依靠带有后缘的自嵌块的锁定功能和自身重量来防止滑动倾覆。该类护岸孔隙间可以人工种植一些植物,增加其美感[3]。混凝土栽植槽是由栽植槽按护岸坡度拼装组成,具有柔性、灵活性较好、生态效果好、防洪能力强、造型多变、对地基要求低的优点,但泥土易被水流带走,造成墙后中空,影响结构的稳定,在水流过急时容易导致墙体垮塌[6]。
关于自重的名言 1、程先生,一个人想得到别人的尊重,就必须先学会自重。 2、自立自重,不可随人脚跟,学人言语。 3、励操行以修法业,当自重;甘淡泊以守清贫,当自省;谋善举以泽众生,当自励。 4、自重、自省、自警、自律,才能保持公仆本色;慎独、慎权、慎欲、慎初,方能抗得住诱惑。 5、人活着,其实就是一种心态,你若觉得快乐,幸福无处不在;你为自己悲鸣,世界必将灰暗。是非常有,不听当无;祸福相依,顺其自然。多行善,福必近;多为恶,祸难远。不奢求,心易安;不冒
进,则身全。心小不容蝼蚁,胸阔能纳百川。顺境淡然,逆境泰然。不自重者取辱,不自足者博学,不自满者受益。 6、不自重者取辱,不自律者招祸,不自满者受益,不自足者博闻。 7、自立自重,不可跟人脚迹,学人言语。陆九渊 8、诚实是力量的一种象征,它显示着一个人的高度自重和内心的安全感与尊严感。艾琳卡瑟 9、人要学会自重,首先要学会不去勉强任何人,包括自己。 10、播种赏识收获自信;播种自信收获自立;播种自重收获自爱;播种激励收获自强。
11、慎独则器自重做会计的人犹要学会慎独。 12、一个正直的人在无论什么地方应该知道自重。巴尔扎克 13、慎言谨行,是修已第一事。不自重者是取辱,不自畏者亦是招祸。 14、自重、自知、自制,惟此三者能使人生达到无上权力之境。但尼生 15、自重是与重大事物有关的品质。一个自重的人具有重大的价值,所以是善良的人。做个真正自重的人是困难的,他须得高尚与善良俱全。他对高贵者矜持,对通常人和蔼。[古希腊]亚里士多德:《尼各马可伦理学》 16、自重、自觉、自制,此三者可以引至生命的崇高境域。丁尼生
热交换器的选型和设计指南
目录 1 概述 (1) 2 换热器的分类及结构特点。 (1) 3 换热器的类型选择 (2) 4 无相变物流换热器的选择 (11) 5 冷凝器的选择 (13) 6 蒸发器的选择 (14) 7 换热器的合理压力降 (17) 8 工艺条件中温度的选用 (18) 9 管壳式换热器接管位置的选取 (19) 10 结构参数的选取 (19) 11 管壳式换热器的设计要点 (23) 12 空冷器的设计要点 (32) 13 空冷器设计基础数据 (35)
1 概述 本工作指南为工艺系统工程师提供换热器的选型原则和工艺参数的选取及计算方法。 2 换热器的分类及结构特点。 表 2-1 换热器的结构分类
3 换热器的类型选择 换热器的类型很多,每种型式都有特定的应用范围。在某一种场合下性能很好的换热器,如果换到另一种场合可能传热效果和性能会有很大的改变。 因此,针对具体情况正确地选择换热器的类型,是很重要的。换热器选型时需要考虑的因素是多方面的,主要有: 1) 热负荷及流量大小 2) 流体的性质 3) 温度、压力及允许压降的范围 4) 对清洗、维修的要求 5) 设备结构、材料、尺寸、重量 6) 价格、使用安全性和寿命 在换热器选型中,除考虑上述因素外,还应对结构强度、材料来源、加工条件、密封性、安全性等方面加以考虑。所有这些又常常是相互制约、相互影响的,通过设计的优化加以解决。针对不同的工艺条件及操作工况,我们有时使用特殊型式的换热器或特殊的换热管,以实现降低成本的目的。因此,应综合考虑工艺条件和机械设计的要求,正确选择合适的换热器型式来有效地减少工艺过程的能量消耗。对工程技术人员而言,在设计换热器时,对于型式的合理选择、经济运行和降低成本等方面应有足够的重视,必要时,还得通过计算来进行技术经济指标分析、投资和操作费用对比,从而使设计达到该具体条件下的最佳设计。 3.1管壳式换热器 管壳式换热器的应用范围很广,适应性很强,其允许压力可以从高真空到41.5MPa,温度可以从-100°C以下到 1100°C高温。此外,它还具有容量
《建筑结构选型》课程教学大纲 课程编号: 610005 课程名称:建筑结构选型 英文名称:Selection of structural design 课程类型: 必修课 总学时:32 讲课学时:32 学分:2 适用对象:建筑学本科 先修课程:无 执笔人:金杰审定人:孟昭博 一.课程性质、目的和任务 《建筑结构选型》课程是建筑学专业学生的一门专业必修课,其基本出发点是紧密结合建筑学专业实际的需要提供相应结构的基本概念知识。 基本目的和意义在于,使学生通过学习后,能掌握基本结构知识,在进行建筑构思和设计中,增强建筑中结构的合理性与可行性,做出比较经济合理、切实可行的建筑方案与设计,以求得建筑艺术与建筑技术的完美结合。同时,加深同学们对一般性房屋结构设计方法的了解,拓宽结构专业方面的知识,开阔学生的眼界和思路。 二.课程教学和教改基本要求 通过学习后,能掌握基本结构知识,在进行建筑构思和设计中,增强建筑中结构的合理性与可行性,做出比较经济合理、切实可行的建筑方案与设计,以求得建筑艺术与建筑技术的完美结合。同时,加深同学们对一般性房屋结构设计方法的了解,拓宽结构专业方面的知识,开阔学生的眼界和思路。 三.课程各章重点与难点、教学要求与教学内容 第一章梁和悬挑构件 教学要求: 了解梁和悬挑构件的形式,掌握梁和悬挑构件的受力及变形特点。 教学重点与难点:梁和悬挑构件的受力及变形特点 教学时数:理论教学2学时。 教学内容: 1.1 梁的形式; 1.按材料来分 (1)石梁, 古代埃及、西亚、希腊形成狭长式密柱林立的空间,如阿蒙神庙,帕提农神庙。 这是因为石村抗弯性能差(抗拉低,抗压高)所以石梁高度很大,极其笨重,跨度受限制, 可达8—9m (2)木梁,
《永葆本色明镜自警》学习心得体会 近期,我通过镇委镇政府组织观看了《永葆本色明镜自警》的警示片,身心又得到了一次震撼,也让自重、自省、自警、自励再次激荡在心间,作为一名党员干部,就是要忠实地贯彻执行党的群众路线。做到权为民所用、情为民所系、利为民所谋,始终不渝地坚持全心全意为人民服务的宗旨,时刻把人民群众的冷暖、忧乐、安危挂在心上: 一、学习廉政规定。通过学习,明白什么能做,什么不能做,脑子里始终要有明确的界限。自觉地以党纪政纪约束自己,用群众的满意程度审视自己,模范地遵守廉洁自律的各项规定;还要学习郑培民、孔繁森等先进人物的事迹,用他们的事迹不断鞭策自己,查找差距,提高觉悟;最后,要用反面典型警醒自己,那些以身试法的人的问题就出在世界观、权力观上,出在缺乏自律意识上,正是由于少了自我学习,自我教育,走上了与人民为敌的邪路。 二、端正生活作风。自觉从工作和生活中的习惯上、小事上反省。我们每一名共产党员一定要在事非原则上泾渭分明,小节上时时刻刻从严把握,干干净净踏踏实实干事,清清白白堂堂正正做人。通过学习,我们要在不断在思想上自
律,在制度面前自律,在监督中自律,在不断经受考验中强化自律。将警钟敲给自己,长鸣不绝于耳,才能有如履薄冰般的谨慎、如临深渊般的警醒。不断要克服贪念,从一个个腐败份子因贪婪而走上穷途末路的人生悲剧里,我们不难发现他们都是贪欲的恶性膨胀而起的。如果他们在生活中培养健康的生活情趣。明白一个党员最基本的价值取向和行为准则,洞察人的某些情趣爱好若处之不慎,就可能变成弱点这些道理,就避免了操守不严、品行不端这些违法违纪现象,近年来暴露的党员干部腐败案,无一例外地印证了这个规律。 三、自觉接受监督。失去监督的权力,必然滋生腐败;脱离监督的干部,往往会犯错误。我们每一名党员干部职工都要正确地对待监督。党组织和群众的监督是一面镜子,经常地照一照,检查一下自己的缺点和不足,及时加以改正和纠正,对自己的成长进步大有裨益。“良药苦口利于病,忠言逆耳利于行”,常被泼点冷水,常听点逆耳之言,可以使头脑保持清醒。加强群众监督,群众永远是一面“镜子”,可以正衣冠正品行;做到自我监督,始终把党纪国法牢记于心,时时拿廉政行为这面“镜子”对照自己。 我们每一个人要从自己的工作性质、业务特点出发,积极主动地承担起反腐倡廉职责。认真学习党的路线方针政
高层宾馆结构选型设计 一、工程概况 为适应城市发展的需要,拟在太原市区某地段内兴建规模为400间客房的高层宾馆一座。总建筑面积为33000㎡,以适应旅游、商务、会议的需要。该宾馆标准不低于三星级酒店标准,占地约15000㎡。 规划要求建筑退让东侧道路红线不得小于10米,退让南侧道路红线不得小于15米;建筑密度不大于,建筑容积率不大于3,绿地率不小于;做好场地的环境设计,组织好交通、人流;规划布局功能分区合理;满足无障碍设计要求;配建停车位,其中地下停车位不少于总停车位的三分之二。包括公共,餐饮,康乐,管理及客房部分,在总图中须布置全部用地范围内之内容,以及道路、绿化、停车场地划分以及、锅炉房、空调机房等设备用空间的布局。 建筑基地位于太原市重要地段,紧邻居住小区以及商业区,周围商业气氛强烈。要求工程功能完善,造型优美,创造都市环境。同时考虑建筑环保、节能方面的技术应用。规划建筑退让东南侧道路红线15m,西南侧道路红线10m。 本次设计对该方案进行结构选型,根据任务书要求,建筑设计概况如下: 占地面积为15000㎡,总建筑面积为㎡,建筑密度,建筑容积率,绿化率%。建筑主体为21层,总高度为,裙房共3层,层高,标准层主体18层,层高。标准客房数310间,双套间30间,三套间10间。标准客房进深,开间。 二、房屋适用高度和高宽比 1、确定抗震设防烈度 抗震设防烈度是按国家规定的权限批准作为一个地区抗震设防依据的地震烈度,一般情况,取50年内超越概率10%的地震烈度。建筑所在地为山西省太原市,根据《建筑抗震设计规范》(GB 50011-2010)确定太原市抗震设防烈度为8度,地震加速度值为。 2、房屋适用高度 初步拟定建筑结构体系为框架-剪力墙结构,根据太原市为8度抗震设防,查表1得此类A级高级钢筋混凝土高层建筑的最大适用高度为100m。该酒店高度为,符合规定要求。 查表2得此类A级高级钢筋混凝土高层建筑的最大高宽比为5。该酒店宽度
关于自省的句子 1、总是失败和总是成功的人最大的区别就是遇到失败的时候是把责任都推到别人身上呢,还是痛定思痛自省己身呢出处:家的n 次方 2、朝省、夕省,朝夕自省;上廉,下廉,上下齐廉。 3、依法行政要牢记职责不辱使命,置身商海应清正廉洁自警自省。 4、做公仆应时时自省三讲,为官者须日日严把三关。 5、领导者应该常常保持自省的姿态和心态。作者:江南春 6、薛之荔:总是失败和总是成功的人最大的区别就是遇到失败的时候是把责任都推到别人身上呢,还是痛定思痛自省己身呢。出处:家的n次方 7、见贤思齐焉,见不贤而内自省也。作者:孔子 8、当我们面对问题时,自省比责怪他人难度要大得多。这也促使多数人选择了更加简单的方式----指责,而犯错的一方自然会选择----反击。这种对立其实没有任何意义!不是吗?每个人做好自己才是重要的。 9、反躬自省是通向美德和上帝的途径。作者:瓦茨 10、飞檐流阁是人们灵魂深处的自省。它的参差错落,结构精巧得厉害。如今亭子有:短亭长亭凉亭茶亭廊亭等等,我更欢喜园子
里的小亭子。那种小模样,惬意而坚韧。 11、被人揭下面具是一种失败,自己揭下面具是一种胜利。作者:雨果 12、人生长路,目的地虽然由不得我们选择,至少在每个路口,该往那走,我们还是可以自己作出判断的。执迷,还是看淡人各有志吧!人生中,我们有许多转念的机会,每个转念都有着我们生活经历的感悟和积累,以及对生命价值的自省。 13、人不知而不温是人生最高修养,自非一时所能达到。对批评家的话我过去并非不加保留,只是增加了我的警惕。即是人言藉藉,自当格外反躬自省,多征求真正内行而寿意的师友的意见。你的自我批评精神,我完全信得过;可是艺术家有时会钻牛角尖而自以为走的是独创而正确的路。要避免这一点,需要经常保持冷静和客观的态度。所谓艺术上的il1usion[幻觉],有时会蒙蔽一个人到几年之久的。至于批评界的黑幕,我近三年译巴尔扎克的《幻灭》,得到不少知识。一世纪前尚且如此,何况今日!二月号《音乐与音乐家》杂志上有一篇karayan[卡拉扬]的访问记,说他对于批评只认为是某先生的意见,如此而已。他对所钦佩的学者,则自会倾听,或者竟自动去请教。这个态度大致与你相仿。出处:傅雷家书 14、我们在人生之路上,如果多些思考,多些自省,多些揣摩,自然也就会多些人生的智慧。铲除一切阻碍,轻装上阵,追逐梦想,让美梦成真。 15、1、一个人彻悟的程度,源于他所受痛苦的程度与自省力,
关于自省的名言警句 1、领导者应该常常保持自省的姿态和心态。江南春 2、共产党员要发挥表率作用,自重、自省、自警、自励,坚定共产主义信念。 3、自重、自省、自警、自励。 4、砺操行以修德业,当自重;甘淡泊以守清贫,当自省;谋善举以泽众生,当自励。 5、薛之荔:总是失败和总是成功的人最大的区别就是遇到失败的时候是把责任都推到别人身上呢,还是痛定思痛自省己身呢。
6、以人为鉴,明白非常,是使人能够反省的妙法。鲁迅 7、朝省、夕省、朝夕自省;上廉、下廉、上下齐廉。 8、自知之明是最难得的知识。西班牙 9、多有不自满的人的种族,永远前进,永远有希望。多有只知责人不知反省的人的种族。祸哉,祸哉!鲁迅 10、自满、自高自大和轻信,是人生的三大暗礁。巴尔扎克 11、见人恶而自省,有则改无则警;见人慕,外则敬内则从。 12、在我们未来的人生道路上,我们应该具备那位先生,那种自省的能力。
13、不会从失败中寻找教训的人,他们的成功之路是遥远的。拿破仑 14、我们应该相比我们优秀的人去学习,正所谓:见贤思齐焉,见不贤而内自省也! 15、学礼仪,见贤思齐,见不贤而自省。 16、大部分人是永远不能被惊醒的怪物,若是给以压力,总会渐行渐远。当外部压力超越内心,他越是心安理得地丧失自我。可当外界心平气和任他内心枝桠蔓延,他却生出了沉重无望的自省与恐惧。 17、勤于学习他人之长的人,是谦逊的人;能够倾听别人意见的人,是明智的人;肯于接受批评的人,是自省的人;善于分析得失的人,是聪明的人;四种品质兼备便成就了包容,有了包容之心,无
论身处顺境逆境,都能怀一颗至真、至美、至善的心,走向最美境界。 18、自省巴换位思考,是你职场交际的秘诀。 19、飞檐流阁是人们灵魂深处的自省。它的参差错落,结构精巧得厉害。如今亭子有:短亭、长亭、凉亭、茶亭、廊亭等等,我更欢喜园子里的小亭子。那种小模样,惬意而坚韧。 20、长大了,该让自己把持着足够多的自知与自省,清醒地知道何时该穿豹纹高跟,何时该穿棉布拖鞋。何时该耀眼,何时该淡然。何时该犀利,何时该温婉。 21、人生,永远是一条漫漫长路,走过了,便领悟了,很多时候对于失去和拥有,都不知是那个,究竟先会来到?或许;太多迷茫里的不知所措,无法去提醒时间里计较的自己,对于某一件自己想去做的事情,又和不做,原本就是两回不相干的事,若让自己能够迅速强大起来,持界竟是选择的境界,懂得彻悟,不断的完善残缺的心智,内修和自省则是自己最好的自律,有时候管好自己就是把握眼前一
关于自省的名言警句大全 1、应该常常保持自省的姿态和心态。江南春 2、*员要发挥表率作用,自重、自省、自警、自励,坚定共产主义信念。 3、自重、自省、自警、自励。 4、砺操行以修德业,当自重;甘淡泊以守清贫,当自省;谋善举以泽众生,当自励。 5、薛之荔:总是失败和总是成功的人的区别就是遇到失败的时候是把责任都推到别人身上呢,还是痛定思痛自省己身呢。 6、以人为鉴,明白非常,是使人能够反省的妙法。鲁迅 7、朝省、夕省、朝夕自省;上廉、下廉、上下齐廉。 8、自知之明是最难得的知识。西班牙
9、多有不自满的人的种族,永远前进,永远有希望。多有只知责人不知反省的人的种族。祸哉,祸哉!鲁迅 10、自满、自高自大和轻信,是人生的三大暗礁。巴尔扎克 11、见人恶而自省,有则改无则警;见人慕,外则敬内则从。 12、在我们未来的人生道路上,我们应该具备那位先生,那种自省的能力。 13、不会从失败中寻找教训的人,他们的成功之路是遥远的。拿破仑 14、我们应该相比我们优秀的人去学习,正所谓:见贤思齐焉,见不贤而内自省也! 15、学礼仪,见贤思齐,见不贤而自省。 16、大部分人是永远不能被惊醒的怪物,若是给以压力,总会渐行渐远。当外部压力超越内心,他越是心安理得地丧失自我。可当外界心平气和任他内心枝桠蔓延,他却生出了沉重无望的自省与恐惧。
17、勤于学习他人之长的人,是谦逊的人;能够倾听别人意见的人,是明智的人;肯于接受批评的人,是自省的人;善于分析得失的人,是聪明的人;四种品质兼备便成就了包容,有了包容之心,无论身处顺境逆境,都能怀一颗至真、至美、至善的心,走向最美境界。 18、自省巴换位思考,是你职场交际的秘诀。 19、飞檐流阁是人们灵魂深处的自省。它的参差错落,结构精巧得厉害。如今亭子有:短亭、长亭、凉亭、茶亭、廊亭等等,我更欢喜园子里的小亭子。那种小模样,惬意而坚韧。 20、长大了,该让自己把持着足够多的自知与自省,清醒地知道何时该穿豹纹高跟,何时该穿棉布拖鞋。何时该耀眼,何时该淡然。何时该犀利,何时该温婉。 21、人生,永远是一条漫漫长路,走过了,便领悟了,很多时候对于失去和拥有,都不知是那个,究竟先会来到?或许;太多迷茫里的不知所措,无法去提醒时间里计较的自己,对于某一件自己想去做的事情,又和不做,原本就是两回不相干的事,若让自己能够迅速强大起来,持界竟是选择的境界,懂得彻悟,不断的完善残缺的心智,内修和自省则
钢结构厂房设计及选型 摘要:随着我国工业经济的飞速发展,各行业厂房设计向着大跨度、大柱距和大吨位方向发展。由于钢结构建筑具有自重轻、承载力强的特点,在大型工业厂房建设中得到了广 泛应用。本文通过分析大型钢结构工业厂房常用的几种结构体系,以某工程为例,针对钢结构的内力设计、节点设计及应用轧制H 型钢设计中的相关问题进行探讨,以期通过本文 的阐述对促进大型钢结构工业厂房建设提供理论参考。 关键字:钢结构厂房 Abstract: with the rapid economic development of our country industry, factory to design various industries large span and large column spacing and the load direction. As the steel structure building has light weight bearing capacity, the characteristics of strong, in large industrial plants has been widely applied in the construction. In this article, through the analysis of large-scale structural steelwork industrial plant commonly used several structure system, and to a project as an example, this paper of the internal force redistribution of the steel structure design, design and application of the node H steel rolling in the design of related problems are discussed, in order to promote the through this paper paper of large steel structure industry plant construction to provide the theory reference. Key word: steel structure plant 中图分类号:[U260.8+1]文献标识码:A 文章编号: 随着社会的发展,技术的进步, 在工业厂房的设计中,钢结构凭借它具有自重轻、造价低、施工周期短、工厂化程度高、现场工作量小、可回收绿色环保、综合效益高等优点,已经成为一种重要的结构形式。本文就结合某工程实例对钢结构厂房的设计阐述一些设计体会。 某工程平面尺寸:横向325m,纵向24+15=39m,檐高17.8m.24米跨间内设50t/10+32/5t(A5)级桥式吊车,15米跨间内设16/3.2t+10t吊车,轻型彩钢屋面,夹芯板外墙。 一、结构方案设计
浅谈高层建筑结构选型及设计 摘要:随着国民经济的快速发展。人民生活水平的不断提高。功能俱全的高层建筑越来越多,而建筑师为了建筑立面美观和艺术上创新,常常使得建筑平面形状和立体的空间形状复杂不规则,建筑体型日趋多样化。本文针对日益复杂的高层建筑结构设计和选型问题进行了分析。 关键词:高层建筑;结构选型;结构设计 abstract: with the rapid development of national economy. the improvement of people’s life. functioning of the high-rise building is more and more, and the architect for the building elevation beautiful and artistic innovation, often made of building plane shapes and stereo space complex shape irregular, building size becoming more diverse. this article in view of the increasingly complex high-rise building structural design and selection problems are analyzed. keywords: high building; the structural type; structure design 中图分类号:[tu208.3]文献标识码:a 文章编号: 随着高层建筑高度、规模、投资与复杂性等逐步增大,结构选型所面临的对象及其所处环境、需考虑解决的问题及所用的知识日趋复杂,结构选型的难度与重要性增大、时间增长,耗费的人力、