ESC GUIDELINES
2015ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation
Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC)
Authors/Task Force Members:Marco Rof?*(Chairperson)(Switzerland),Carlo Patrono *(Co-Chairperson)(Italy),Jean-Philippe Collet ?(France),Christian Mueller ?(Switzerland),Marco Valgimigli ?(The Netherlands),
Felicita Andreotti (Italy),Jeroen J.Bax (The Netherlands),Michael A.Borger (Germany),Carlos Brotons (Spain),Derek P.Chew (Australia),Baris Gencer (Switzerland),Gerd Hasenfuss (Germany),Keld Kjeldsen (Denmark),
Patrizio Lancellotti (Belgium),Ulf Landmesser (Germany),Julinda Mehilli (Germany),Debabrata Mukherjee (USA),Robert F.Storey (UK),and Stephan Windecker (Switzerland)
Document Reviewers:Helmut Baumgartner (CPG Review Coordinator)(Germany),Oliver Gaemperli (CPG Review Coordinator)(Switzerland),Stephan Achenbach (Germany),Stefan Agewall (Norway),Lina Badimon (Spain),
Colin Baigent (UK),He
′ctor Bueno (Spain),Raffaele Bugiardini (Italy),Scipione Carerj (Italy),Filip Casselman (Belgium),Thomas Cuisset (France),?etin Erol (Turkey),Donna Fitzsimons (UK),Martin Halle
(Germany),
*Corresponding authors:Marco Rof?,Division of Cardiology,University Hospital,Rue Gabrielle Perret-Gentil 4,1211Geneva 14,Switzerland,Tel:+41223723743,Fax:+41223727229,E-mail:Marco.Rof?@hcuge.ch
Carlo Patrono,Istituto di Farmacologia,Universita
`Cattolica del Sacro Cuore,Largo F.Vito 1,IT-00168Rome,Italy,Tel:+390630154253,Fax:+39063050159,E-mail:carlo.patrono@rm.unicatt.it
&The European Society of Cardiology 2015.All rights reserved.For permissions please email:journals.permissions@https://www.doczj.com/doc/e314967604.html,.
?
Section Coordinators af?liations listed in the Appendix.
ESC Committee for Practice Guidelines (CPG)and National Cardiac Societies document reviewers listed in the Appendix.ESC entities having participated in the development of this document:
Associations:Acute Cardiovascular Care Association (ACCA),European Association for Cardiovascular Prevention &Rehabilitation (EACPR),European Association of Cardiovas-cular Imaging (EACVI),European Association of Percutaneous Cardiovascular Interventions (EAPCI),Heart Failure Association (HFA).
Councils:Council on Cardiovascular Nursing and Allied Professions (CCNAP),Council for Cardiology Practice (CCP),Council on Cardiovascular Primary Care (CCPC).Working Groups:Working Group on Cardiovascular Pharmacotherapy,Working Group on Cardiovascular Surgery,Working Group on Coronary Pathophysiology and Microcir-culation,Working Group on Thrombosis.
The content of these European Society of Cardiology (ESC)Guidelines has been published for personal and educational use only.No commercial use is authorized.No part of the ESC Guidelines may be translated or reproduced in any form without written permission from the ESC.Permission can be obtained upon submission of a written request to Oxford University Press,the publisher of the European Heart Journal and the party authorized to handle such permissions on behalf of the ESC.
Disclaimer:The ESC Guidelines represent the views of the ESC and were produced after careful consideration of the scienti?c and medical knowledge and the evidence available at the time of their publication.The ESC is not responsible in the event of any contradiction,discrepancy and/or ambiguity between the ESC Guidelines and any other of?cial recom-mendations or guidelines issued by the relevant public health authorities,in particular in relation to good use of healthcare or therapeutic strategies.Health professionals are encour-aged to take the ESC Guidelines fully into account when exercising their clinical judgment,as well as in the determination and the implementation of preventive,diagnostic or therapeutic medical strategies;however,the ESC Guidelines do not override,in any way whatsoever,the individual responsibility of health professionals to make appropriate and accurate decisions in consideration of each patient’s health condition and in consultation with that patient and,where appropriate and/or necessary,the patient’s caregiver.Nor do the ESC Guidelines exempt health professionals from taking into full and careful consideration the relevant of?cial updated recommendations or guidelines issued by the competent public health authorities,in order to manage each patient’s case in light of the scienti?cally accepted data pursuant to their respective ethical and professional obligations.It is also the health professional’s responsibility to verify the applicable rules and regulations relating to drugs and medical devices at the time of prescription.
European Heart Journal
doi:10.1093/eurheartj/ehv320
European Heart Journal Advance Access published September 11, 2015 by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
Christian Hamm (Germany),David Hildick-Smith (UK),Kurt Huber (Austria),Efstathios Iliodromitis (Greece),Stefan James (Sweden),Basil S.Lewis (Israel),Gregory Y.H.Lip (UK),Massimo F.Piepoli (Italy),Dimitrios Richter (Greece),Thomas Rosemann (Switzerland),Udo Sechtem (Germany),Ph.Gabriel Steg (France),Christian Vrints (Belgium),and Jose Luis Zamorano (Spain)
The disclosure forms of all experts involved in the development of these guidelines are available on the ESC website https://www.doczj.com/doc/e314967604.html,/guidelines
------------------------------------------------------------------------------------------------------------------------------------------------------Keywords
Acute cardiac care ?Acute coronary syndromes ?Angioplasty ?Anticoagulation ?Apixaban ?Aspirin ?Atherothrombosis ?Beta-blockers ?Bivalirudin ?Bypass surgery ?Cangrelor ?Chest pain unit ?Clopidogrel ?Dabigatran ?Diabetes ?Early invasive strategy ?Enoxaparin ?European Society of Cardiology ?Fondaparinux ?Glycoprotein IIb/IIIa inhibitors ?Guidelines ?Heparin ?High-sensitivity troponin ?Myocardial ischaemia ?Nitrates ?Non-ST-elevation myocardial infarction ?Platelet inhibition ?Prasugrel ?Recommendations ?Revascularization ?Rhythm monitoring ?Rivaroxaban ?Statin ?Stent ?Ticagrelor ?Unstable angina ?Vorapaxar
Table of Contents
Abbreviations and acronyms ........................41.Preamble ...................................52.Introduction .................................
72.1De?nitions,pathophysiology and epidemiology .......72.1.1Universal de?nition of myocardial infarction ......72.1.1.1Type 1MI .........................72.1.1.2Type 2MI .........................72.1.2Unstable angina in the era of high-sensitivity cardiac troponin assays ............................72.1.3Pathophysiology and epidemiology
(see Web addenda).........................73.Diagnosis ...................................
73.1Clinical presentation ........................73.2Physical examination ........................83.3Diagnostic tools ...........................83.3.1Electrocardiogram ......................83.3.2Biomarkers ...........................93.3.3‘Rule-in’and ‘rule-out’algorithms .............103.3.4Non-invasive imaging .....................113.3.4.1Functional evaluation ..................113.3.4.2Anatomical evaluation .................113.4Differential diagnosis ........................124.Risk assessment and outcomes .....................
124.1Clinical presentation,electrocardiogram and biomarkers 124.1.1Clinical presentation .....................124.1.2Electrocardiogram ......................124.1.3Biomarkers ...........................134.2Ischaemic risk assessment.....................134.2.1Acute risk assessment ....................134.2.2Cardiac rhythm monitoring.................134.2.3Long-term risk .........................144.3Bleeding risk assessment (14)
4.4Recommendations for diagnosis,risk strati?cation,imaging and rhythm monitoring in patients with suspected non-ST-elevation acute coronary syndromes ................14
5.Treatment ..................................
155.1Pharmacological treatment of ischaemia ...........
15
5.1.1General supportive measures ...............155.1.2Nitrates .............................155.1.3Beta-blockers..........................155.1.4Other drug classes (see Web addenda) (16)
5.1.5Recommendations for anti-ischaemic drugs in the acute phase of non-ST-elevation acute coronary syndromes ...............................165.2Platelet inhibition ..........................165.2.1Aspirin ..............................165.2.2P2Y 12inhibitors ........................165.2.2.1Clopidogrel ........................165.2.2.2Prasugrel ..........................165.2.2.3Ticagrelor .........................175.2.2.4Cangrelor .........................185.2.3Timing of P2Y 12inhibitor administration ........195.2.4Monitoring of P2Y 12inhibitors
(see Web addenda).........................195.2.5Premature discontinuation of oral antiplatelet therapy..................................195.2.6Duration of dual antiplatelet therapy...........195.2.7Glycoprotein IIb/IIIa inhibitors ...............205.2.7.1Upstream versus procedural initiation (see Web addenda)........................205.2.7.2Combination with P2Y 12inhibitors
(see Web addenda)........................205.2.7.3Adjunctive anticoagulant therapy
(see Web addenda)........................205.2.8Vorapaxar (see Web addenda)..............205.2.9Recommendations for platelet inhibition in non-ST-elevation acute coronary syndromes .........205.3Anticoagulation ...........................215.3.1Anticoagulation during the acute phase .........215.3.1.1Unfractionated heparin ................215.3.1.2Low molecular weight heparin ............225.3.1.3Fondaparinux .......................225.3.1.4Bivalirudin .........................225.3.2Anticoagulation following the acute phase ...
....
23
ESC Guidelines
Page 2of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
non-ST-elevation acute coronary syndromes (23)
5.4Managing oral antiplatelet agents in patients requiring
long-term oral anticoagulants (24)
5.4.1Patients undergoing percutaneous coronary intervention (24)
5.4.2Patients medically managed or requiring coronary
artery bypass surgery (26)
5.4.3Recommendations for combining antiplatelet agents
and anticoagulants in non-ST-elevation acute coronary syndrome patients requiring chronic oral anticoagulation.26 5.5Management of acute bleeding events
(see Web addenda) (27)
5.5.1General supportive measures(see Web addenda)..27 5.5.2Bleeding events on antiplatelet agents
(see Web addenda) (27)
5.5.3Bleeding events on vitamin K antagonists
(see Web addenda) (27)
5.5.4Bleeding events on non-vitamin K antagonist oral anticoagulants(see Web addenda) (27)
5.5.5Non-access-related bleeding events
(see Web addenda) (27)
5.5.6Bleeding events related to percutaneous coronary intervention(see Web addenda) (27)
5.5.7Bleeding events related to coronary artery bypass surgery(see Web addenda) (27)
5.5.8Transfusion therapy(see Web addenda) (27)
5.5.9Recommendations for bleeding management and
blood transfusion in non-ST-elevation acute coronary syndromes (27)
5.6Invasive coronary angiography and revascularization (28)
5.6.1Invasive coronary angiography (28)
5.6.1.1Pattern of coronary artery disease (28)
5.6.1.2Identi?cation of the culprit lesion (28)
5.6.1.3Fractional?ow reserve (29)
5.6.2Routine invasive vs.selective invasive approach (29)
5.6.3Timing of invasive strategy (29)
5.6.3.1Immediate invasive strategy(,2h) (29)
5.6.3.2Early invasive strategy(,24h) (29)
5.6.3.3Invasive strategy(,72h) (30)
5.6.3.4Selective invasive strategy (31)
5.6.4Conservative treatment (31)
5.6.4.1In patients with coronary artery disease (31)
5.6.4.1.1Non-obstructive CAD (31)
5.6.4.1.2CAD not amenable to revascularization (31)
5.6.4.2In patients with normal coronary angiogram
(see Web addenda) (31)
5.6.5Percutaneous coronary intervention (31)
5.6.5.1Technical aspects and challenges (31)
5.6.5.2Vascular access (32)
5.6.5.3Revascularization strategies and outcomes (32)
5.6.6Coronary artery bypass surgery (32)
5.6.6.1Timing of surgery and antithrombotic drug
discontinuation(see Web addenda) (33)
5.6.6.2Recommendations for perioperative
management of antiplatelet therapy in non-ST-elevation
artery bypass surgery (33)
5.6.6.3Technical aspects and outcomes
(see Web addenda) (33)
5.6.7Percutaneous coronary intervention vs.coronary
artery bypass surgery (33)
5.6.8Management of patients with cardiogenic shock (34)
5.6.9Recommendations for invasive coronary angiography
and revascularization in non-ST-elevation acute coronary syndromes (34)
5.7Gender speci?cities(see Web addenda) (35)
5.8Special populations and conditions(see Web addenda).35
5.8.1The elderly and frail patients(see Web addenda)..35
5.8.1.1Recommendations for the management of
elderly patients with non-ST-elevation acute coronary
syndromes (35)
5.8.2Diabetes mellitus(see Web addenda) (35)
5.8.2.1Recommendations for the management of
diabetic patients with non-ST-elevation acute coronary
syndromes (35)
5.8.3Chronic kidney disease(see Web addenda) (36)
5.8.3.1Dose adjustment of antithrombotic agents
(see Web addenda) (36)
5.8.3.2Recommendations for the management of
patients with chronic kidney disease and non-ST-
elevation acute coronary systems (36)
5.8.4Left ventricular dysfunction and heart failure(see
Web addenda) (36)
5.8.4.1Recommendations for the management of
patients with acute heart failure in the setting of non-ST-
elevation acute coronary syndromes (36)
5.8.4.2Recommendations for the management of
patients with heart failure following non-ST-elevation
acute coronary syndromes (37)
5.8.5Atrial?brillation(see Web addenda) (37)
5.8.5.1Recommendations for the management of atrial
?brillation in patients with non-ST-elevation acute
coronary syndromes (37)
5.8.6Anaemia(see Web addenda) (38)
5.8.7Thrombocytopenia(see Web addenda) (38)
5.8.7.1Thrombocytopenia related to GPIIb/IIIa
inhibitors(Web addenda) (38)
5.8.7.2Heparin-induced thrombocytopenia(Web
addenda) (38)
5.8.7.3Recommendations for the management of
thrombocytopenia in non-ST-elevation acute coronary
syndromes (38)
5.8.8Patients requiring chronic analgesic or anti-
in?ammatory treatment(see Web addenda) (38)
5.8.9Non-cardiac surgery(see Web addenda) (38)
5.9Long-term management (38)
5.9.1Medical therapy for secondary prevention (38)
5.9.1.1Lipid-lowering treatment (38)
5.9.1.2Antithrombotic therapy (38)
5.9.1.3ACE inhibition (38)
5.9.1.4Beta-blockers (38)
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/
Downloaded from
5.9.1.7Glucose-lowering therapy in diabetic patients..38
5.9.2Lifestyle changes and cardiac rehabilitation (39)
5.9.3Recommendations for long-term management after
non-ST-elevation acute coronary syndromes (39)
6.Performance measures (39)
7.Summary of management strategy (40)
8.Gaps in evidence (41)
9.To do and not to do messages from the guidelines (42)
10.Web addenda and companion documents (43)
11.Acknowledgements (43)
12.Appendix (43)
13.References (43)
Abbreviations and acronyms
ACC American College of Cardiology ACCOAST Comparison of Prasugrel at the Time of
Percutaneous Coronary Intervention or as
Pretreatment at the Time of Diagnosis in
Patients with Non-ST Elevation Myocardial
Infarction
ACE angiotensin-converting enzyme
ACS acute coronary syndromes
ACT activated clotting time
ACTION Acute Coronary Treatment and Intervention
Outcomes Network
ACUITY Acute Catheterization and Urgent Interven-
tion Triage strategY
ADAPT-DES Assessment of Dual AntiPlatelet Therapy with
Drug-Eluting Stents
ADP adenosine diphosphate
AHA American Heart Association
APPRAISE Apixaban for Prevention of Acute Ischaemic
Events
aPTT activated partial thromboplastin time
ARB angiotensin receptor blocker
ATLAS ACS 2-TIMI51Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Aspirin With or With-out Thienopyridine Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction51
ATP adenosine triphosphate
BARC Bleeding Academic Research Consortium BMS bare-metal stent
CABG coronary artery bypass graft
CAD coronary artery disease
CHA2DS2-VASc Cardiac failure,Hypertension,Age≥75
(2points),Diabetes,Stroke(2points)–
Vascular disease,Age65–74,Sex category CHAMPION Cangrelor versus Standard Therapy to
Achieve Optimal Management of Platelet
Inhibition
CI con?dence interval
CK creatine kinase COX cyclooxygenase
CMR cardiac magnetic resonance
CPG Committee for Practice Guidelines
CREDO Clopidogrel for the Reduction of Events
During Observation
CRUSADE Can Rapid risk strati?cation of Unstable an-
gina patients Suppress ADverse outcomes
with Early implementation of the ACC/AHA
guidelines
CT computed tomography
CURE Clopidogrel in Unstable Angina to Prevent
Recurrent Events
CURRENT-OASIS
7
Clopidogrel and Aspirin Optimal Dose Usage
to Reduce Recurrent Events–Seventh Organ-
ization to Assess Strategies in Ischaemic
Syndromes
CV cardiovascular
CYP cytochrome P450
DAPT dual(oral)antiplatelet therapy
DES drug-eluting stent
EARLY-ACS Early Glycoprotein IIb/IIIa Inhibition in
Non-ST-Segment Elevation Acute Coronary
Syndrome
ECG electrocardiogram
eGFR estimated glomerular?ltration rate
EMA European Medicines Agency
ESC European Society of Cardiology
FDA Food and Drug Administration
FFR fractional?ow reserve
FREEDOM Future Revascularization Evaluation in
Patients with Diabetes Mellitus:Optimal
Management of Multivessel Disease
GPIIb/IIIa glycoprotein IIb/IIIa
GRACE2.0Global Registry of Acute Coronary Events2.0
GUSTO Global Utilization of Streptokinase and TPA
for Occluded Arteries
GWTG Get With The Guidelines
HAS-BLED hypertension,abnormal renal and liver func-
tion(1point each),stroke,bleeding history
or predisposition,labile INR,elderly(.65
years),drugs and alcohol(1point each)
HIT heparin-induced thrombocytopenia
HORIZONS Harmonizing Outcomes with Revasculariza-
tiON and Stents in Acute Myocardial Infarction
HR hazard ratio
IABP-Shock II Intra-Aortic Balloon Pump in Cardiogenic
Shock II
IMPROVE-IT IMProved Reduction of Outcomes:Vytorin
Ef?cacy International Trial
INR international normalized ratio
ISAR-CLOSURE Instrumental Sealing of ARterial puncture
site–CLOSURE device versus manual
compression
ISAR-REACT Intracoronary stenting and Antithrombotic
Regimen–Rapid Early Action for Coronary
Treatment
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/
Downloaded from
ISAR-TRIPLE Triple Therapy in Patients on Oral Anticoagula-tion After Drug Eluting Stent Implantation i.v.intravenous
LDL low-density lipoprotein
LMWH low molecular weight heparin LV left ventricular
LVEF left ventricular ejection fraction MACE major adverse cardiovascular event
MATRIX
Minimizing Adverse Haemorrhagic Events by TRansradial Access Site and Systemic Imple-mentation of angioX
MDCT multidetector computed tomography
MERLIN
Metabolic Ef?ciency With Ranolazine for Less Ischaemia in Non-ST-Elevation Acute Coron-ary Syndromes
MI myocardial infarction
MINAP Myocardial Infarction National Audit Project NOAC non-vitamin K antagonist oral anticoagulant NSAID non-steroidal anti-in?ammatory drug
NSTE-ACS non-ST-elevation acute coronary syndromes NSTEMI non-ST-elevation myocardial infarction NYHA New York Heart Association OAC oral anticoagulation/anticoagulant
OASIS Organization to Assess Strategies for Ischae-mic Syndromes OR
odds ratio
PARADIGM-HF
Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure
PCI
percutaneous coronary intervention
PEGASUS-TIMI 54
Prevention of Cardiovascular Events in Pa-tients with Prior Heart Attack Using Ticagre-lor Compared to Placebo on a Background of Aspirin-Thrombolysis in Myocardial Infarction 54
PLATO PLATelet inhibition and patient Outcomes POISE PeriOperative ISchemic Evaluation RCT randomized controlled trial
RIVAL RadIal Vs femorAL access for coronary intervention RR relative risk
RRR
relative risk reduction
SAFE-PCI Study of Access Site for Enhancement of PCI for Women s.c.subcutaneous
STEMI
ST-segment elevation myocardial infarction SWEDEHEART
Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recom-mended Therapies
SYNERGY
Superior Yield of the New Strategy of Enoxa-parin,Revascularization and Glycoprotein IIb/IIIa Inhibitors trial
SYNTAX SYNergy between percutaneous coronary intervention with TAXus and cardiac surgery TACTICS
Treat angina with Aggrastat and determine Cost of Therapy with an Invasive or Conser-vative Strategy
TIA transient ischaemic attack
TIMACS Timing of Intervention in Patients with Acute Coronary Syndromes
TIMI
Thrombolysis In Myocardial Infarction
TRA 2P-TIMI 50
Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events–Thrombolysis in Myocardial Infarc-tion 50
TRACER
Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome
TRILOGY ACS
Targeted Platelet Inhibition to Clarify the Op-timal Strategy to Medically Manage Acute Coronary Syndromes
TRITON-TIMI 38
TRial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet InhibitioN with Prasugrel–Thrombolysis In Myocardial Infarction 38
TVR target vessel revascularization UFH unfractionated heparin VKA vitamin K antagonist
WOEST
What is the Optimal antiplatElet and anti-coagulant therapy in patients with OAC and coronary StenTing
ZEUS
Zotarolimus-eluting Endeavor Sprint Stent in Uncertain DES Candidates
1.Preamble
Guidelines summarize and evaluate all available evidence on a par-ticular issue at the time of the writing process,with the aim of assist-ing health professionals in selecting the best management strategies for an individual patient with a given condition,taking into account the impact on outcome,as well as the risk–bene?t ratio of particu-lar diagnostic or therapeutic means.Guidelines and recommenda-tions should help health professionals to make decisions in their daily practice.However,the ?nal decisions concerning an individual patient must be made by the responsible health professional(s)in consultation with the patient and caregiver as appropriate.
A great number of Guidelines have been issued in recent years by the European Society of Cardiology (ESC)as well as by other soci-eties and organisations.Because of the impact on clinical practice,quality criteria for the development of guidelines have been estab-lished in order to make all decisions transparent to the user.The re-commendations for formulating and issuing ESC Guidelines can be found on the ESC website (https://www.doczj.com/doc/e314967604.html,/Guidelines-&-Education/Clinical-Practice-Guidelines/Guidelines-development/Writing-ESC-Guidelines ).ESC Guidelines represent the of?cial pos-ition of the ESC on a given topic and are regularly updated.
Members of this Task Force were selected by the ESC to re-present professionals involved with the medical care of patients with this pathology.Selected experts in the ?eld undertook a com-prehensive review of the published evidence for management (including diagnosis,treatment,prevention and rehabilitation)of a given condition according to ESC Committee for Practice Guide-lines (CPG)policy.A critical evaluation of diagnostic and therapeutic procedures was performed,including assessment of the
ESC Guidelines
Page 5of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
risk–bene?t ratio.Estimates of expected health outcomes for larger populations were included,where data exist.The level of evidence and the strength of the recommendation of particular management options were weighed and graded according to prede?ned scales,as outlined in Tables 1and 2.
The experts of the writing and reviewing panels provided declar-ation of interest forms for all relationships that might be perceived as real or potential sources of con?icts of interest.These forms were compiled into one ?le and can be found on the ESC website (https://www.doczj.com/doc/e314967604.html,/guidelines ).Any changes in declarations of interest that arise during the writing period must be noti?ed to the ESC and updated.The Task Force received its entire ?nancial support from the ESC without any involvement from the healthcare industry.
The ESC CPG supervises and coordinates the preparation of new Guidelines produced by task forces,expert groups or consensus pa-nels.The Committee is also responsible for the endorsement pro-cess of these Guidelines.The ESC Guidelines undergo extensive review by the CPG and external experts.After appropriate revi-sions the Guidelines are approved by all the experts involved in the Task Force.The ?nalized document is approved by the CPG for publication in the European Heart Journal.The Guidelines were developed after careful consideration of the scienti?c and medical knowledge and the evidence available at the time of their dating.
The task of developing ESC Guidelines covers not only integration of the most recent research,but also the creation of educational tools and implementation programmes for the recom-mendations.To implement the guidelines,condensed pocket guidelines versions,summary slides,booklets with essential mes-sages,summary cards for non-specialists and an electronic version for digital applications (smartphones,etc.)are produced.These versions are abridged and thus,if needed,one should always refer to the full text version which is freely available on the ESC website.
The National Societies of the ESC are encouraged to endorse,translate and implement all ESC Guidelines.Implementation pro-grammes are needed because it has been shown that the outcome of disease may be favourably in?uenced by the thorough applica-tion of clinical recommendations.
Surveys and registries are needed to verify that real-life daily prac-tice is in keeping with what is recommended in the guidelines,thus completing the loop between clinical research,writing of guidelines,disseminating them and implementing them into clinical practice.Health professionals are encouraged to take the ESC Guidelines fully into account when exercising their clinical judgment,as well as in the determination and the implementation of preventive,diagnos-tic or therapeutic medical strategies.However,the ESC Guidelines do not override in any way whatsoever the individual responsibility of health professionals to make appropriate and accurate decisions in consideration of each patient’s health condition and in consult-ation with that patient and the patient’s caregiver where appropriate and/or necessary.It is also the health professional’s responsibility to verify the rules and regulations applicable to drugs and devices at the time of prescription.
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
2.Introduction
2.1De?nitions,pathophysiology and epidemiology
The leading symptom that initiates the diagnostic and therapeutic cascade in patients with suspected acute coronary syndromes (ACS)is chest pain.Based on the electrocardiogram (ECG),two groups of patients should be differentiated:
(1)Patients with acute chest pain and persistent (.20min)
ST-segment elevation.
This condition is termed ST-elevation ACS and generally re-?ects an acute total coronary occlusion.Most patients will ultim-ately develop an ST-elevation myocardial infarction (STEMI).The mainstay of treatment in these patients is immediate reperfusion by primary angioplasty or ?brinolytic therapy.1
(2)Patients with acute chest pain but no persistent ST-segment
elevation.
ECG changes may include transient ST-segment elevation,persistent or transient ST-segment depression,T-wave inver-sion,?at T waves or pseudo-normalization of T waves or the ECG may be normal.The clinical spectrum of non-ST-elevation ACS (NSTE-ACS)may range from patients free of symptoms at presentation to individuals with ongoing ischaemia,electrical or haemodynamic instability or cardiac arrest.The pathological correlate at the myocardial level is cardiomyocyte necrosis [NSTE-myocardial infarction (NSTEMI)]or,less frequently,myocardial ischaemia without cell loss (unstable angina).A small proportion of patients may present with ongoing myocardial ischaemia,characterized by one or more of the follow-ing:recurrent or ongoing chest pain,marked ST depression on 12-lead ECG,heart failure and haemodynamic or electrical instabil-ity.Due to the amount of myocardium in jeopardy and the risk of malignant ventricular arrhythmias,immediate coronary angiography and,if appropriate,revascularization are indicated.
2.1.1Universal de?nition of myocardial infarction
Acute myocardial infarction (MI)de?nes cardiomyocyte necrosis in a clinical setting consistent with acute myocardial ischaemia.2A combination of criteria is required to meet the diagnosis of acute MI,namely the detection of an increase and/or decrease of a cardiac biomarker,preferably high-sensitivity cardiac troponin,with at least one value above the 99th percentile of the upper reference limit and at least one of the following:
(1)Symptoms of ischaemia.
(2)New or presumed new signi?cant ST-T wave changes or left
bundle branch block on 12-lead ECG.
(3)Development of pathological Q waves on ECG.
(4)Imaging evidence of new or presumed new loss of viable myo-cardium or regional wall motion abnormality.
(5)Intracoronary thrombus detected on angiography or autopsy.2.1.1.1Type 1MI
Type 1MI is characterized by atherosclerotic plaque rupture,ulcer-ation,?ssure,erosion or dissection with resulting intraluminal thrombus in one or more coronary arteries leading to decreased
myocardial blood ?ow and/or distal embolization and subsequent myocardial necrosis.The patient may have underlying severe coron-ary artery disease (CAD)but,on occasion (i.e.5–20%of cases),there may be non-obstructive coronary atherosclerosis or no angio-graphic evidence of CAD,particularly in women.2–5
2.1.1.2Type 2MI
Type 2MI is myocardial necrosis in which a condition other than cor-onary plaque instability contributes to an imbalance between myo-cardial oxygen supply and demand.2Mechanisms include coronary artery spasm,coronary endothelial dysfunction,tachyarrhythmias,bradyarrhythmias,anaemia,respiratory failure,hypotension and se-vere hypertension.In addition,in critically ill patients and in patients undergoing major non-cardiac surgery,myocardial necrosis may be related to injurious effects of pharmacological agents and toxins.6
The universal de?nition of MI also includes type 3MI (MI resulting in death when biomarkers are not available)and type 4and 5MI (related to percutaneous coronary intervention [PCI]and coronary artery bypass grafting [CABG],respectively).
2.1.2Unstable angina in the era of high-sensitivity cardiac troponin assays
Unstable angina is de?ned as myocardial ischaemia at rest or minimal exertion in the absence of cardiomyocyte necrosis.Among unse-lected patients presenting with suspected NSTE-ACS to the emer-gency department,the introduction of high-sensitivity cardiac troponin measurements in place of standard troponin assays resulted in an increase in the detection of MI ( 4%absolute and 20%relative increase)and a reciprocal decrease in the diagnosis of unstable an-gina.7–10Compared with NSTEMI patients,individuals with unstable angina do not experience myocardial necrosis,have a substantially lower risk of death and appear to derive less bene?t from intensi?ed antiplatelet therapy as well as early invasive strategy.2–4,6–132.1.3Pathophysiology and epidemiology (see Web addenda)
3.Diagnosis
3.1Clinical presentation
Anginal pain in NSTE-ACS patients may have the following presentations:
?Prolonged (.20min)anginal pain at rest;
?New onset (de novo)angina (class II or III of the Canadian Car-diovascular Society classi?cation);21
?Recent destabilization of previously stable angina with at least Canadian Cardiovascular Society Class III angina characteristics (crescendo angina);or ?Post-MI angina.
Prolonged and de novo/crescendo angina are observed in 80%and 20%of patients,respectively.Typical chest pain is character-ized by a retrosternal sensation of pressure or heaviness (‘angina’)radiating to the left arm (less frequently to both arms or to the right arm),neck or jaw,which may be intermittent (usually lasting several minutes)or persistent.Additional symptoms such as sweating,nau-sea,abdominal pain,dyspnoea and syncope may be present.Atypical
ESC Guidelines
Page 7of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
isolated dyspnoea.Atypical complaints are more often observed in the elderly,in women and in patients with diabetes,chronic renal disease or dementia.22–24The exacerbation of symptoms by phys-ical exertion and their relief at rest increase the probability of myo-cardial ischaemia.The relief of symptoms after nitrates administration is not speci?c for anginal pain as it is reported also in other causes of acute chest pain.24In patients presenting with sus-pected MI to the emergency department,overall,the diagnostic per-formance of chest pain characteristics for MI is limited.24Older age,male gender,family history of CAD,diabetes,hyperlipidaemia,hypertension,renal insuf?ciency,previous manifestation of CAD as well as peripheral or carotid artery disease increase the likelihood of NSTE-ACS.Conditions that may exacerbate or precipitate NSTE-ACS include anaemia,infection,in?ammation,fever,and metabolic or endocrine (in particular thyroid)disorders.
3.2Physical examination
Physical examination is frequently unremarkable in patients with suspected NSTE-ACS.Signs of heart failure or haemodynamic or electrical instability mandate a quick diagnosis and treatment.Car-diac auscultation may reveal a systolic murmur due to ischaemic mi-tral regurgitation,which is associated with poor prognosis,or aortic
mechanical complication (i.e.papillary muscle rupture or ventricular septal defect)of a subacute and possibly undetected MI.Physical examination may identify signs of non-coronary causes of chest pain (e.g.pulmonary embolism,acute aortic syndromes,myoperi-carditis,aortic stenosis)or extracardiac pathologies (e.g.pneumo-thorax,pneumonia or musculoskeletal diseases).In this setting,the presence of a chest pain that can be reproduced by exerting pressure on the chest wall has a relatively high negative predictive value for NSTE-ACS.24,26According to the presentation,abdominal disorders (e.g.oesophageal spasm,oesophagitis,gastric ulcer,chole-cystitis,pancreatitis)may also be considered in the differential diag-nosis.Differences in blood pressure between the upper and lower limbs or between the arms,irregular pulse,jugular vein distension,heart murmurs,friction rub and pain reproduced by chest or ab-dominal palpation are ?ndings suggestive of alternative diagnoses.Pallor,sweating or tremor may point towards precipitating condi-tions such as anaemia and thyrotoxicosis.27
3.3Diagnostic tools
3.3.1Electrocardiogram
The resting 12-lead ECG is the ?rst-line diagnostic tool in the assess-ment of patients with suspected ACS (Figure 1).It is recommended to
High Likelihood Low Likelihood Low Likelihoo o d High Likelihoo
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
immediate reperfusion.1Comparison with previous tracings is valuable,particularly in patients with pre-existing ECG abnormal-ities.It is recommended to obtain additional12-lead ECGs in the case of persistent or recurrent symptoms or diagnostic uncer-tainty.In patients with bundle branch block or paced rhythm, ECG is of no help for the diagnosis of NSTE-ACS.
3.3.2Biomarkers
Biomarkers complement clinical assessment and12-lead ECG in the diagnosis,risk strati?cation and treatment of patients with suspected NSTE-ACS.Measurement of a biomarker of cardiomyocyte injury, preferably high-sensitivity cardiac troponin,is mandatory in all pa-tients with suspected NSTE-ACS.2,6,8Cardiac troponins are more sensitive and speci?c markers of cardiomyocyte injury than creatine kinase(CK),its MB isoenzyme(CK-MB)and myoglobin.6If the clin-ical presentation is compatible with myocardial ischaemia,then a dy-namic elevation of cardiac troponin above the99th percentile of healthy individuals indicates MI.2In patients with MI,levels of cardiac troponin rise rapidly(https://www.doczj.com/doc/e314967604.html,ually within1h if using high-sensitivity as-says)after symptom onset and remain elevated for a variable period of time(usually several days).2,6Advances in technology have led to a re?nement in cardiac troponin assays and have improved the ability to detect and quantify cardiomyocyte injury.2,6,8,10,29–37In Europe,recommended over less sensitive ones.2,6,8The majority of currently
used point-of-care assays cannot be considered sensitive or high-sensitivity assays.8,35Therefore the obvious advantage of
point-of-care tests,namely the shorter turnaround time,is counter-balanced by lower sensitivity,lower diagnostic accuracy and lower negative predictive value.Overall,automated assays have been
more thoroughly evaluated as compared with point-of-care tests.2,6,8
As these techniques continue to improve and performance charac-teristics are both assay and hospital dependent,no recommendation regarding the site of measurement(central laboratory vs.bedside)
can be given.2,6,8,38Data from large multicentre studies have consist-
ently shown that sensitive and high-sensitivity cardiac troponin as-
says increase diagnostic accuracy for MI at the time of presentation
as compared with conventional assays,especially in patients present-
ing early after chest pain onset,and allow for a more rapid‘rule-in’
and‘rule-out’of MI(see section3.3.3and Table3).2,6,8,29–34
In most patients with renal dysfunction,elevations in cardiac tropo-
nin should not be primarily attributed to impaired clearance and con-sidered harmless,as cardiac conditions such as chronic coronary or hypertensive heart disease seem to be the most important contribu-
tor to troponin elevation in this setting.41Other life-threatening con-
ditions presenting with chest pain,such as aortic dissection and pulmonary embolism,may also result in elevated troponin levels
and should be considered as differential diagnoses(Table4).
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/
Downloaded from
Among the multitude of additional biomarkers evaluated for the
diagnosis of NSTE-ACS,only CK-MB and copeptin seem to have clinical relevance.2,6,8,10,44–50CK-MB shows a more rapid decline after MI as compared with cardiac troponin and may provide added value for the timing of myocardial injury and the detection of early reinfarction.2,6,8,10Assessment of copeptin,the C-terminal part of the vasopressin prohormone,may quantify the endogenous stress level in multiple medical conditions including MI.As the level of en-dogenous stress appears to be invariably high at the onset of MI,the added value of copeptin to conventional (less sensitive)cardiac troponin assays is substantial.44–50Therefore the routine use of copeptin as an additional biomarker for the early rule-out of MI is recommended whenever sensitive or high-sensitivity cardiac troponin assays are not available.Copeptin may have some added value even over high-sensitivity cardiac troponin in the early rule-out of MI.44–48
3.3.3‘Rule-in’and ‘rule-out’algorithms
Due to the higher sensitivity and diagnostic accuracy for the detec-tion of acute MI at presentation,the time interval to the second car-diac troponin assessment can be shortened with the use of high-sensitivity assays.This may reduce substantially the delay to diagnosis,translating into shorter stays in the emergency depart-ment and lower costs.2,6,8,10,29–36It is recommended to use the 0h/3h algorithm (Figure 2).As an alternative,0h/1h assessments are recommended when high-sensitivity cardiac troponin assays with a validated algorithm are available (Figure 3).The 0h/1h algo-rithms rely on two concepts:?rst,high-sensitivity cardiac troponin is a continuous variable and the probability of MI increases with in-creasing high-sensitivity cardiac troponin values;39second,early ab-solute changes of the levels within 1h can be used as surrogates for
absolute changes over 3h or 6h and provide incremental diagnostic value to the cardiac troponin assessment at presentation.39The cut-off levels within the 0h/1h algorithm are assay speci?c.36,39,51–55
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
Those algorithms should always be integrated with a detailed clinical assessment and 12-lead ECG and repeat blood sampling is mandatory in case of ongoing or recurrent chest pain (Table 5,see Web addenda).
Table 5(see Web addenda)Characteristics of the 0h/3h and 0h/1h algorithms
The negative predictive value for MI in patients assigned ‘rule-out’exceeded 98%in several large validation cohorts.30–34,36,39,51–55Used in conjunction with clinical and ECG ?ndings,the 0h/1h algorithm may allow the identi?cation of candidates for early dis-charge and outpatient management.The positive predictive value for MI in those patients meeting the ‘rule-in’criteria was 75–80%.30–34,39,53–55Most of the ‘rule-in’patients with diagnoses other than MI did have conditions that usually require inpatient coronary angiography for accurate diagnosis,including Tako–Tsubo cardio-myopathy and myocarditis.39,53–55Patients who do not qualify for ‘rule-out’or ‘rule-in’represent a heterogeneous group that may re-quire further investigations if no alternative explanation for the car-diac troponin elevation is identi?ed.A large proportion of these patients may require a further high-sensitivity cardiac troponin as-sessment (e.g.at 3h).Coronary angiography should be considered in patients for whom there is a high degree of clinical suspicion of NSTE-ACS,while in patients with low to intermediate likelihood for this condition,computed tomography (CT)coronary angiog-raphy should be considered.No further diagnostic testing in the emergency department is indicated when alternative conditions such as rapid ventricular rate response to atrial ?brillation or hyper-tensive emergency have been identi?ed.
For rapid rule-out,two alternative approaches to the 0h/1h or 0h/3h algorithms have been adequately validated and may be considered.First,a 2h rule-out protocol combining the Thromboly-sis in Myocardial Infarction (TIMI)risk score with ECG and high-sensitivity cardiac troponin at presentation allowed a safe rule-out in up to 40%of patients.56–58Second,a dual-marker strategy com-bining normal levels of cardiac troponin together with low levels of copeptin (,10pmol/L)at presentation showed very high negative predictive value for MI,obviating the need for serial testing in se-lected patients.44–50When using any algorithm,three main caveats apply:(i)algorithms should only be used in conjunction with all avail-able clinical information,including detailed assessment of chest pain characteristics and ECG;(ii)in patients presenting very early (e.g.within 1h from chest pain onset),the second cardiac troponin level should be obtained at 3h,due to the time dependency of troponin release;(iii)as late increases in cardiac troponin have been de-scribed in 1%of patients,serial cardiac troponin testing should be pursued if the clinical suspicion remains high or whenever the pa-tient develops recurrent chest pain.52,54High-sensitivity cardiac troponin assays also maintain high diagnostic accuracy in patients with renal dysfunction.To ensure the best possible clinical use,assay-speci?c optimal cut-off levels,which are higher in patients with renal dysfunction,should be used.593.3.4Non-invasive imaging
3.3.
4.1Functional evaluation
Transthoracic echocardiography should be routinely available in emergency rooms and chest pain units and performed/interpreted
by trained physicians in all patients during hospitalization for NSTE-ACS .This imaging modality is useful to identify abnormalities suggestive of myocardial ischaemia or necrosis (i.e.segmental hypo-kinesia or akinesia).In the absence of signi?cant wall motion abnor-malities,impaired myocardial perfusion detected by contrast echocardiography or reduced regional function using strain and strain rate imaging might improve the diagnostic and prognostic va-lue of conventional echocardiography.60,61Moreover,echocardiog-raphy can help in detecting alternative pathologies associated with chest pain,such as acute aortic dissection,pericardial effusion,aortic valve stenosis,hypertrophic cardiomyopathy or right ventricular dilatation suggestive of acute pulmonary embolism.Similarly,echo-cardiography is the diagnostic tool of choice for patients with haemodynamic instability of suspected cardiac origin.62Evaluation of left ventricular (LV)systolic function,at the latest by the time of hospital discharge,is important to estimate prognosis,and echo-cardiography (as well as other imaging modalities)can provide this information.
In patients without ischaemic changes on 12-lead ECGs and nega-tive cardiac troponins (preferably high-sensitivity)who are free of chest pain for several hours,stress imaging can be performed during admission or shortly after discharge.Stress imaging is preferred over exercise ECG due to its greater diagnostic accuracy.63Various studies have shown that normal exercise,dobutamine or dipyridamole stress echocardiograms have high negative predictive value for ischaemia and are associated with excellent patient outcomes.64,65Moreover,stress echocardiography demonstrated superior prognostic value over exer-cise ECG.64,66The addition of contrast may improve endocardial bor-der detection,which may facilitate detection of ischaemia.67
Cardiac magnetic resonance (CMR)can assess both perfusion and wall motion abnormalities,and patients presenting with acute chest pain with a normal stress CMR have an excellent short-and midterm prognosis.68CMR also permits detection of scar tissue (using late gadolinium enhancement)and can differentiate this from recent infarction (using T2-weighted imaging to delineate myo-cardial oedema).69,70Moreover,CMR can facilitate the differential diagnosis between infarction and myocarditis or Tako–Tsubo car-diomyopathy.71Similarly,nuclear myocardial perfusion imaging has been shown to be useful for risk strati?cation of patients with acute chest pain suggestive for ACS.Resting myocardial scintigraphy,by detecting ?xed perfusion defects suggestive of myocardial necrosis,can be helpful for initial triage of patients presenting with chest pain without ECG changes or elevated cardiac troponins.72Combined stress–rest imaging may further enhance assessment of ischaemia,while a normal study is associated with excellent outcome.73,74Stress–rest imaging modalities are usually not widely available on 24h service.
3.3.
4.2Anatomical evaluation
Multidetector computed tomography (MDCT)allows for visualiza-tion of the coronary arteries and a normal scan excludes CAD.A meta-analysis of nine studies (n ?1349patients)has reported over-all high negative predictive values to exclude ACS (by excluding CAD)and excellent outcome in patients presenting to the emer-gency department with low to intermediate pre-test probability for ACS and a normal coronary CT angiogram.75Four randomized controlled trials (RCTs)have tested MDCT (n ?1869patients)vs.
ESC Guidelines
Page 11of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
usual care (n ?1397)in the triage of low-to intermediate-risk pa-tients presenting with acute chest pain to emergency departments without signs of ischaemia on ECG and/or inconclusive cardiac tro-ponins.76–79At a follow-up of 1–6months,there were no deaths,and a meta-analysis demonstrated comparable outcomes with the two approaches (i.e.no difference in the incidence of MI,post-discharge emergency department visits or rehospitalizations)and showed that MDCT was associated with a reduction in emergency de-partment costs and length of stay.80However,none of these studies used high-sensitivity cardiac troponin assays,which also may reduce hospital stay.It was also noted that MDCT was associated with an in-crease in the use of invasive angiography {8.4%vs.6.3%;odds ratio [OR]1.36[95%con?dence interval (CI)1.03,1.80],P ?0.030}.80Ac-cordingly,MDCT coronary angiography can be used to exclude CAD (and MDCT is thus not useful in patients with known CAD).Other factors limiting MDCT coronary angiography include severe calci?ca-tions (high calcium score)and elevated or irregular heart rate;in add-ition,a suf?cient level of expertise is needed and 24h service is currently not widely available.Finally,the use of MDCT coronary angi-ography in the acute setting in patients with stents or previous CABG has not been validated.Importantly,CT imaging can effectively exclude other causes of acute chest pain that,if untreated,are associated with high mortality,namely pulmonary embolism,aortic dissection and ten-sion pneumothorax.81
3.4Differential diagnosis
Among unselected patients presenting with acute chest pain to the emergency department,disease prevalence can be expected to be the following:5–10%STEMI,15–20%NSTEMI,10%unstable an-gina,15%other cardiac conditions and 50%non-cardiac dis-eases.48,51,52,56–58Several cardiac and non-cardiac conditions may mimic NSTE-ACS (Table 6).
Conditions that should always be considered in the differential diagnosis of NSTE-ACS,because they are potentially life-threatening but also treatable,include aortic dissection,pulmonary embolism and tension pneumothorax.Echocardiography should be performed urgently in all patients with haemodynamic instability of suspected cardiovascular (CV)origin.62
Chest X-ray is recommended in all patients in whom NSTE-ACS is considered unlikely in order to detect pneumonia,pneumothorax,rib fractures or other thoracic disorders.Tako–Tsubo cardiomyopathy and coronary artery spasm are brie?y described in section 5.6.4.2,Web addenda.Stroke may be accompanied by ECG changes,myo-cardial wall motion abnormalities and an increase in cardiac troponin levels.2,6The majority of patients presenting with acute chest pain to the emergency department have non-cardiac conditions causing the chest discomfort.In many instances the pain is musculoskeletal,and therefore benign,self-limiting and does not require hospitalization.Chest pain characteristics help to some extent in the early identi?ca-tion of those patients.24
4.Risk assessment and outcomes
4.1Clinical presentation,
electrocardiogram and biomarkers
4.1.1Clinical presentation
In addition to some universal clinical markers of risk,such as ad-vanced age,diabetes and renal insuf?ciency,the initial clinical pres-entation is highly predictive of early prognosis.82Chest pain at rest carries a worse prognosis than symptoms elicited during physical exertion.In patients with intermittent symptoms,an increasing number of episodes preceding the index event also adversely affects prognosis.Tachycardia,hypotension,heart failure and new mitral regurgitation at presentation predict poor prognosis and call for ra-pid diagnosis and management.25,82–84
4.1.2Electrocardiogram
The initial ECG is predictive of early risk.18Patients with ST depres-sion have a worse prognosis than patients with a normal ECG.85,86The number of leads showing ST depression and the magnitude of ST depression are indicative of the extent of ischaemia and correlate with prognosis on the one hand,and bene?t from an invasive treat-ment strategy on the other.87ST depression ≥0.05mV in two or more contiguous leads,in the appropriate clinical context,is sug-gestive of NSTE-ACS and linked to adverse prognosis.85ST depres-sion combined with transient ST elevation identi?es a high-risk subgroup,88while associated T-wave inversion does not alter the prognostic value of ST depression.While isolated T-wave inversion on admission has not been associated with worse prognosis com-pared with the absence of ECG abnormalities,it frequently triggers a more rapid diagnosis and treatment.86
ESC Guidelines
Page 12of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
4.1.3Biomarkers
Beyond diagnostic utility,cardiac troponin levels add prognostic in-formation in terms of short-and long-term mortality to clinical and ECG variables.While high-sensitivity cardiac troponin T and I seem to have comparable diagnostic accuracy,high-sensitivity cardiac troponin T has greater prognostic accuracy.89,90The higher the high-sensitivity troponin levels at presentation,the greater the risk of death.6,8,10,39Multiple biomarkers have been associated with mortality in NSTE-ACS,several of them conferring additive prognostic value to cardiac troponin.8,48–50Serum creatinine and estimated glomerular ?ltration rate (eGFR)should also be deter-mined in all patients with NSTE-ACS because they affect prognosis and are key elements of the Global Registry of Acute Coronary Events (GRACE 2.0)risk calculation (see section 4.2).The exten-sively validated natriuretic peptides (i.e.B-type natriuretic peptide,N-terminal pro-B-type natriuretic peptide and midregional pro-A-type natriuretic peptide)provide prognostic information on top of cardiac troponin.91To some extent,the same applies to high-sensitivity C-reactive protein and novel biomarkers such as midre-gional pro-adrenomedullin,growth differentiation factor 15and copeptin.However,the assessment of these markers has so far not been shown to improve patient management and their added value in risk assessment on top of the GRACE 2.0risk calculation seems marginal.Therefore the routine use of these biomarkers for prognos-tic purposes cannot be recommended at the present time.
4.2Ischaemic risk assessment
In NSTE-ACS,quantitative assessment of ischaemic risk by means of scores is superior to the clinical assessment alone.The GRACE risk score provides the most accurate strati?cation of risk both on ad-mission and at discharge.92,93The GRACE 2.0risk calculator (https://www.doczj.com/doc/e314967604.html,/WebSite/default.aspx?ReturnUrl=%2f )pro-vides a direct estimation,bypassing the calculation of a score,of mortality while in hospital,at 6months,at 1year and at 3years.The combined risk of death or MI at 1year is also provided.94Variables used in the GRACE 2.0risk calculation include age,systolic blood pressure,pulse rate,serum creatinine,Killip class at presenta-tion,cardiac arrest at admission,elevated cardiac biomarkers and ST deviation.If the Killip class or serum creatinine values are not avail-able,a modi?ed score can be calculated by adding renal failure and use of diuretics,respectively.The TIMI risk score uses seven vari-ables in an additive scoring system:age ≥65years,three or more CAD risk factors,known CAD,aspirin use in the past 7days,severe angina (two or more episodes within 24h),ST change ≥0.5mm and positive cardiac marker (https://www.doczj.com/doc/e314967604.html,/index.php?page=calculators).82It is simple to use,but its discriminative accuracy is in-ferior to that of the GRACE risk score and the GRACE 2.0risk cal-culation.While the value of risk scores as prognostic assessment tools is undisputed,the impact of risk score implementation on pa-tient outcomes has not been adequately investigated.95,96
4.2.1Acute risk assessment
Patients with suspected NSTE-ACS must be evaluated rapidly in order to identify individuals with ongoing myocardial ischaemia who are at risk of life-threatening arrhythmias and need close surveillance as well as immediate coronary angiography.Patients with suspected NSTE-ACS should be observed in interdisciplinary emergency depart-ments or chest pain units until the diagnosis of MI is con?rmed or ruled
out.The greatest challenge is the integration of clinical presentation with information derived from ECG,troponin assessment and imaging modalities into a standardised management strategy.97Assessment of acute risk guides initial evaluation,selection of the site of care (i.e.cor-onary or intensive care unit,intermediate care unit,inpatient moni-tored unit or regular unit)and therapy,including antithrombotic treatment and timing of coronary angiography.Risk is highest at the time of presentation and may remain elevated for several days,al-though rapidly declining over time,depending on clinical presentation,comorbidities,coronary anatomy and revascularization.98The esti-mated risk should be communicated to the patient and their family.
4.2.2Cardiac rhythm monitoring
Early revascularization as well as the use of antithrombotic agents and beta-blockers have markedly reduced the incidence of life-threatening arrhythmias in the acute phase to ,3%,with most of the arrhythmic events occurring within 12h of symptom on-set.99,100Patients with life-threatening arrhythmias more frequently had prior heart failure,LV ejection fraction (LVEF),30%and triple-vessel CAD.A patient with NSTE-ACS who presents early after symptom onset,has no or mild to moderate cardiac biomarker ele-vation,normal LV function and single-vessel CAD successfully trea-ted with PCI may be discharged the next day.At the other end of the spectrum are NSTE-ACS patients with multivessel CAD in whom complete revascularization may not be achieved in one session (or at all);these patients may have a complicated course (e.g.heart failure)or prior cardiac disease,major comorbidities,advanced age or recent extensive myocardial necrosis.101,102Cardiac troponin-negative (i.e.unstable angina)patients without recurrent or ongoing symptoms and with normal ECG do not necessarily require rhythm monitoring or hospital admission.
NSTEMI patients at low risk for cardiac arrhythmias require rhythm monitoring for ≤24h or until coronary revascularization (whichever comes ?rst)in an intermediate or coronary care unit,while individuals at intermediate to high risk for cardiac arrhythmia may require rhythm monitoring for .24h in an intensive or coronary care unit or in an intermediate care unit,depending on the clinical presentation,degree of revascularization and early post-revascularization course (Table 7).It is recommended that per-sonnel adequately equipped and trained to manage life-threatening ESC Guidelines
Page 13of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
arrhythmias and cardiac arrest accompany patients who are trans-ferred between facilities during the time window in which they re-quire continuous rhythm monitoring.
4.2.3Long-term risk
In addition to short-term risk factors,a number of conditions are as-sociated with long-term risk,including a complicated clinical course,LV systolic dysfunction,atrial ?brillation,severity of CAD,revascu-larization status,evidence of residual ischaemia on non-invasive test-ing and non-cardiac comorbidities.At 1year,the rates of death,MI and recurrent ACS in contemporary NSTE-ACS registries are .10%.While early events are related to ruptured coronary plaques and associated thrombosis,the majority of later events may be the result of coronary and systemic atherosclerosis progression.98,103
4.3Bleeding risk assessment
Major bleeding events are associated with increased mortality in NSTE-ACS.104,105Bleeding risk scores have been developed from registry or trial cohorts in the setting of ACS and PCI.The Can Rapid risk strati?cation of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE)bleeding risk score (https://www.doczj.com/doc/e314967604.html, )was developed from a cohort of 71277NSTE-ACS patients (derivation cohort)and further validated in a co-hort of 17857patients (validation cohort)from the same registry.106The CRUSADE bleeding risk score considered baseline patient char-acteristics (i.e.female gender,history of diabetes,history of peripheral vascular disease or stroke),admission clinical variables (i.e.heart rate,systolic blood pressure,signs of heart failure)and admission labora-tory values (i.e.haematocrit,calculated creatinine clearance)to esti-mate the patient’s likelihood of an in-hospital major bleeding event.However,model performance for the risk score was modest (C-statistic 0.68in patients treated conservatively and 0.73in patients undergoing invasive approach).
The Acute Catheterization and Urgent Intervention Triage strat-egY (ACUITY)bleeding risk score was derived from a pooled cohort of 17421patients with ACS (both NSTE-ACS and STEMI)recruited in the ACUITY and Harmonizing Outcomes with RevasculariZatiON and Stents in Acute Myocardial Infarction (HORIZONS-AMI)trials.104Six independent baseline predictors (i.e.female gender,advanced age,elevated serum creatinine,white blood cell count,anaemia and presentation as NSTEMI or STEMI)and one treat-ment-related variable [use of unfractionated heparin (UFH)and a glycoprotein IIb/IIIa (GPIIb/IIIa)inhibitor rather than bivalirudin alone]were identi?ed.This risk score identi?ed patients at increased risk for non-CABG-related major bleeds at 30days and subsequent 1year mortality.However,it has not been validated in an independent co-hort,no risk calculator is available and model performance for the risk score is modest (C-statistic 0.74).Changes in interventional practice,such as increasing use of radial access,reduction in the dose of UFH,use of bivalirudin,diminished use of GPIIb/IIIa inhibitors and adminis-tration of more effective inhibitors of the platelet adenosine diphos-phate (ADP)receptor P2Y 12(P2Y 12inhibitors),may all modify the predictive value of risk scores.Ischaemic and bleeding risks need to be weighed in the individual patient,although many of the predictors of ischaemic events are also associated with bleeding complica-tions.104,106Overall,CRUSADE and ACUITY scores have reasonable predictive value for major bleeding in ACS patients undergoing
coronary angiography,with CRUSADE found to be the most discrim-inatory.107However,in patients medically treated or on oral anticoa-gulants,the predictive value of these scores is not established.Moreover,the impact on patient outcomes of integrating these scores has not been investigated.Given these limitations,use of the CRUSADE bleeding risk score may be considered in patients under-going coronary angiography to quantify bleeding risk.
4.4Recommendations for diagnosis,risk strati?cation,imaging and rhythm monitoring in patients with suspected non-ST-elevation acute coronary syndromes
ESC Guidelines
Page 14of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
5.1.4
Other drug classes (see Web addenda)
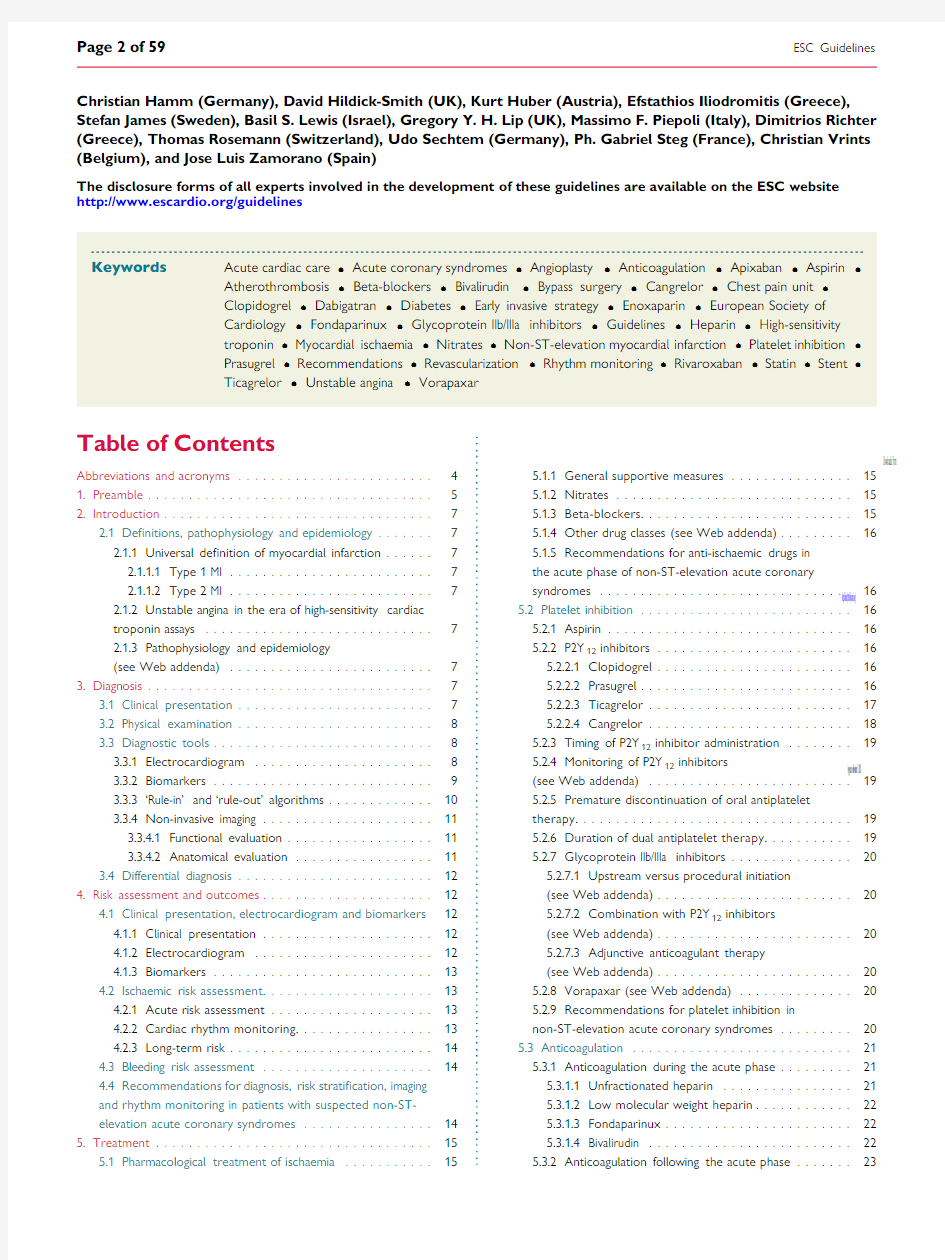
5.1.5Recommendations for anti-ischaemic drugs in the acute phase of non-ST-elevation acute coronary syndromes synthase 1(COX-1),thereby suppressing thromboxane A 2pro-duction throughout the platelet lifespan.128Aspirin has been shown to be effective in patients with unstable angina;the incidence of MI or death was consistently reduced in four RCTs in the pre-PCI era.129–132A meta-analysis of these trials suggests that aspirin administration (up to 2years)is associated with a highly sig-ni?cant 46%odds reduction in major vascular events.133The Clopi-dogrel and Aspirin Optimal Dose Usage to Reduce Recurrent Events–Seventh Organization to Assess Strategies in Ischaemic Syn-dromes (CURRENT-OASIS 7),which enrolled 25086ACS (both NSTE-ACS and STEMI)patients undergoing invasive strategy,found no difference between higher-dose (300–325mg/day)and lower-dose (75–100mg/day)aspirin.134An oral loading dose (150–300mg)of plain aspirin (non-enteric-coated formulation)is recom-mended,while the recommended intravenous (i.v.)dose is 150mg.No monitoring of its effects is required.The mechanisms of action of antiplatelet and anticoagulant agents are described in Figure 4.5.2.2P2Y 12inhibitors 5.2.2.1Clopidogrel
Clopidogrel (300–600mg loading and 75mg/day maintenance dose)is an inactive prodrug that requires oxidation by the hepatic
cytochrome P450(CYP)system to generate an active metabolite (Ta-ble 8).An estimated 85%of the prodrug is hydrolysed by esterases into an inactive form,leaving only 15%of clopidogrel available for to the active metabolite,which selectively and irre-inactivates platelet P2Y 12receptors and thus inhibits platelet aggregation.135,136Dual antiplatelet therapy aspirin and clopidogrel has been shown to reduce ischaemic events in the NSTE-ACS setting compared with 137,138However,up to 10%of patients treated with the of aspirin and clopidogrel will have a recurrent ischaemic ?rst year after an ACS,with a rate of stent thrombosis of 139This residual risk may be partly explained by suboptimal due to inadequate response to clopidogrel.Indeed,and pharmacokinetic studies have described sub-variability in the antiplatelet response to this an increased risk of ischaemic and bleeding events in clopi-and hyper-responders,respectively.140–143There is evi-key gene polymorphisms are involved in both the of active metabolite generation and clinical ef?cacy of clo-–147
(60mg loading and 10mg/day maintenance dose)is a pro-irreversibly blocks platelet P2Y 12receptors with a faster a more profound inhibitory effect than clopidogrel This compound has been tested against the 300mg load-mg/day maintenance dose of clopidogrel in the TRial to in Therapeutic Outcomes by Optimizing InhibitioN with Prasugrel –Thrombolysis In Myocardial (TRITON-TIMI 38),in which ACS patients (STEMI and scheduled for PCI received the drugs during or after 148In the 10074NSTE-ACS patients included,recur-events were reduced in prasugrel-treated patients at the follow-up [from 11.2%to 9.3%;relative risk (RR)0.820.73,0.93),P ?0.002],driven by a signi?cant reduction 9.2%to 7.1%;RRR 23.9%(95%CI 12.7,33.7),P ,0.001].Severe bleeding complications were more common with prasugrel [TIMI non-CABG major bleeds 2.4%vs.1.8%;hazard ratio (HR)1.40(95%CI 1.05,1.88),P ?0.02],due to an increase in spon-taneous bleeds [1.6%vs.1.1%;HR 1.51(95%CI 1.09,2.08),P ?0.01]and fatal bleeds [0.4%vs.0.1%;HR 4.19(95%CI 1.58,11.11),P ?0.002].149Bleeding events were increased by more than four-fold in prasugrel-treated patients referred for early CABG.Based on the marked reduction in de?nite or probable stent thrombosis observed in the TRITON-TIMI 38overall [1.13%in the prasugrel arm vs.2.35%in the clopidogrel arm;HR 0.48(95%CI 0.36,0.64),P ,0.0001]and in patients with drug-eluting stents (DESs)[0.84%vs.2.31%,respectively;HR 0.36(95%CI 0.22,0.58),P ,0.0001],prasugrel should be considered in patients who present with stent thrombosis despite compliance with clo-pidogrel therapy.150,151Prasugrel is contraindicated in patients with prior stroke/transient ischaemic attack (TIA)due to evidence of net harm in this group in TRITON-TIMI 38.In addition,the study showed no apparent bene?t in patients .75years of age or with low bodyweight (,60kg).148The Targeted Platelet Inhib-ition to Clarify the Optimal Strategy to Medically Manage Acute Coronary Syndromes (TRILOGY ACS)trial is discussed in section 5.6.4.1.1.
ESC Guidelines
Page 16of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
5.2.2.3Ticagrelor
Ticagrelor is an oral,reversibly binding P2Y 12inhibitor with a plasma half-life of 6–12h.Ticagrelor also inhibits adenosine reuptake via equilabrative nucleoside transporter 1(ENT1)(Table 8).Like prasu-grel,ticagrelor has a more rapid and consistent onset of action com-pared with clopidogrel,as well as a faster offset of action with more rapid recovery of platelet function.152Ticagrelor increases levels of drugs metabolized through CYP3A,such as simvastatin,while mod-erate CYP3A inhibitors,such as diltiazem,increase ticagrelor plasma levels and might delay the offset of effect.In the PLATelet inhibition and patient Outcomes (PLATO)trial,18624patients with moderate-to high-risk NSTE-ACS (planned for either conservative or invasive management)or STEMI were randomized to either clo-pidogrel 75mg/day,with a loading dose of 300–600mg,
or
ADP = adenosine diphosphate; AT = antithrombin; GP = glycoprotein; LMWH = low molecular weight heparin; Tx = thromboxane;UFH = Unfractionated heparin. Vorapaxar is a protease-activated receptor 1 (PAR1) blocker.
Figure 4Antithrombotic drugs for non-ST-elevation acute coronary syndromes.The ?gure depicts the targets of available antithrombotic
drugs that can be used to inhibit blood coagulation and platelet aggregation during and after thrombus formation.
ESC Guidelines
Page 17of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
ticagrelor 180mg loading dose followed by 90mg twice a day.153Patients undergoing PCI were allowed to receive an additional blinded 300mg loading dose of clopidogrel (total loading dose 600mg)or its placebo.Treatment was continued for up to 12months,with a median duration of drug exposure of 9months.153In the NSTE-ACS subgroup (n ?11080),the primary composite ef-?cacy endpoint (death from CV causes,MI or stroke)was signi?-cantly reduced with ticagrelor compared with clopidogrel [10.0%vs.12.3%;HR 0.83(95%CI 0.74,0.93),P ?0.0013]with similar re-ductions for CV death [3.7%vs.4.9%;HR 0.77(95%CI 0.64,0.93),P ?0.0070]and all-cause mortality [4.3%vs.5.8%;HR 0.76(95%CI 0.64,0.90),P ?0.0020].154Differences in bleeding event rates were also similar in the NSTE-ACS subgroup compared with the overall study,with increased risk of non-CABG-related PLATO-de?ned major bleeds with ticagrelor compared with clopidogrel [4.8%vs.3.8%;HR 1.28(95%CI 1.05,1.56),P ?0.0139]but no difference in life-threatening or fatal bleeds.154The bene?ts of ticagrelor com-pared with clopidogrel in NSTE-ACS were independent of whether or not revascularization was performed in the ?rst 10days after ran-domization.154The reduction in de?nite stent thrombosis with tica-grelor in the NSTE-ACS subgroup [1.1%vs.1.4%;HR 0.71(95%CI 0.43,1.17]was consistent with that seen in the trial overall [1.4%vs.1.9%;HR 0.67(95%CI 0.50,0.90),P ?0.0091].155In addition to in-creased rates of minor or non-CABG-related major bleeding events with ticagrelor,adverse effects included dyspnoea (without bronchospasm),increased frequency of asymptomatic ventricular pauses and increases in uric acid.153,156
5.2.2.4Cangrelor
Cangrelor is an i.v.adenosine triphosphate (ATP)analogue that binds reversibly and with high af?nity to the platelet P2Y 12receptor and has a short plasma half-life (,10min)(Table 8).It produces a highly ef-fective inhibition of ADP-induced platelet aggregation immediately after i.v.bolus administration and allows for restoration of platelet function within 1–2h of infusion discontinuation in NSTE-ACS pa-tients.157Cangrelor (30m g/kg bolus and 4m g/kg/min infusion)in-itiated at the commencement of PCI has been examined in three clinical trials including a total of 24910patients:one with clopidogrel (600mg)given at the beginning of PCI [Cangrelor versus Standard Therapy to Achieve Optimal Management of Platelet Inhibition (CHAMPION)-PCI],one with clopidogrel (600mg)initiated at the end of PCI (CHAMPION-PLATFORM),and one with clopidogrel (300or 600mg)initiated either before or after PCI based on local clinical practice (CHAMPION-PHOENIX)among patients without prior P2Y 12or GPIIb/IIIa inhibition.158–160A meta-analysis of these studies,in which 69%of patients were undergoing PCI for ACS,ob-served a 19%RRR in periprocedural death,MI,ischaemia-driven re-vascularization and stent thrombosis [cangrelor 3.8%vs.clopidogrel 4.7%;OR 0.81(95%CI 0.71,0.91),P ?0.007],with a 39%RRR in stent thrombosis alone [cangrelor 0.5%vs.clopidogrel 0.8%;OR 0.61(95%CI 0.43,0.80),P ?0.008].161The combination of TIMI ma-jor and minor bleeds was increased [cangrelor 0.9%vs.clopidogrel 0.6%;OR 1.38(95%CI 1.03,1.86),P ?0.007],but there was no in-crease in the rate of transfusions.The European Commission issued marketing authorization for this compound in March 2015.
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
5.2.3Timing of P2Y 12inhibitor administration
Initiation of P2Y 12inhibitors soon after the diagnosis of NSTE-ACS irrespective of management strategy has been recommended.162,163This implies pretreatment,de?ned as P2Y 12inhibitor administration before coronary angiography,in patients scheduled for an invasive approach.Subsequently the results of the only RCT on P2Y 12inhibi-tor pretreatment in NSTE-ACS,the Comparison of Prasugrel at the Time of Percutaneous Coronary Intervention or as Pretreatment at the Time of Diagnosis in Patients with Non-ST Elevation Myocardial Infarction (ACCOAST)trial,were published.164The ACCOAST study compared pretreatment with prasugrel 30mg and a further 30mg dose prior to PCI with a regimen of prasugrel 60mg after diagnostic angiography but prior to PCI among 4033patients with NSTEMI scheduled for early invasive strategy.The median duration of pretreatment was 4.3h.Sixty-nine per cent of the patients under-went PCI,6%required surgical revascularization and the remainder were treated conservatively.164At 7days,patients randomized to the pretreatment arm experienced no reduction in the primary end-point (i.e.CV death,recurrent MI,stroke,urgent revascularization and bailout use of GPIIb/IIIa inhibitors)[HR 1.02(95%CI 0.84,1.25),P ?0.81],and no bene?ts emerged at 30days.164TIMI major bleeds were signi?cantly increased in the pretreatment group at 7days [pretreatment 2.6%vs.no pretreatment 1.4%;HR 1.90,(95%CI 1.19,3.02),P ?0.006].Arguments for and against pretreat-ment with P2Y 12inhibitors in NSTE-ACS patients have been dis-cussed extensively and the topic remains controversial.165,166As the optimal timing of ticagrelor or clopidogrel administration in NSTE-ACS patients scheduled for an invasive strategy has not been adequately investigated,no recommendation for or against pretreat-ment with these agents can be formulated.Based on the ACCOAST results,pretreatment with prasugrel is not recommended.In NSTE-ACS patients planned for conservative management,P2Y 12in-hibition (preferably with ticagrelor)is recommended,in the absence of contraindications,as soon as the diagnosis is con?rmed.5.2.4Monitoring of P2Y 12inhibitors (see Web addenda)5.2.5Premature discontinuation of oral antiplatelet therapy
Withdrawal of oral antiplatelet therapy may lead to an increased risk of recurrent events,particularly when the recommended course of therapy has not yet been completed.176–178Interruption of DAPT soon after stent implantation increases the risk of stent thrombosis,especially within the ?rst month after cessation.178While discontinu-ation of DAPT prior to cardiac surgery is discussed in sections 5.6.6.1Web addenda and 5.6.6.2,in the case of a non-cardiac surgical proced-ure that cannot be postponed,a minimum of 1and 3months DAPT for bare-metal stents (BMSs)and new-generation DESs,respectively,might be acceptable.179In this setting,surgery should be performed in hospitals having continuous catheterization laboratory availability,so as to treat patients immediately in case of perioperative MI.179If inter-ruption of DAPT becomes mandatory because of urgent high-risk surgery (e.g.neurosurgery)or in the case of a major bleed that cannot be controlled by local treatment,no alternative therapy can be pro-posed as a substitute to DAPT to prevent stent thrombosis.Low mo-lecular weight heparin (LMWH)has been advocated,but the proof of ef?cacy for this indication is lacking.180Whenever possible,aspirin should be continued because early discontinuation of both antiplate-let drugs will further increase the risk of stent thrombosis.
In patients undergoing elective non-cardiac surgery,ticagrelor and clopidogrel should be discontinued 5days before surgery,while the interval should be increased to 7days in patients on prasugrel,unless the patient is at high risk of stent thrombosis.179In the latter case,a multidisciplinary decision is required to determine the best strategy.Longer discontinuation times (e.g.7days for ticagrelor and 10days for clopidogrel or prasugrel)may be appropriate for surgery at extreme risk of bleeding (e.g.some types of neurosur-gery).For NSTE-ACS patients,the risk of bleeds related to surgery must be balanced against the risk of recurrent ischaemic events related to discontinuation of therapy.The type of surgery,the is-chaemic risk and extent of CAD,the time since the acute episode and,for patients who have undergone PCI,the time since the pro-cedure and the type of stent implanted are key elements of the dis-cussion.Selected patients who require non-cardiac surgery after recently implanted stents may bene?t from bridging therapy with small molecule GPIIb/IIIa inhibitors (i.e.tiro?ban or epti?batide)after discontinuation of the P2Y 12inhibitor,while cangrelor has so far been tested as bridging therapy to CABG.181,182In patients on DAPT following an episode of NSTE-ACS that was treated conser-vatively,the P2Y 12inhibitor may be discontinued.In surgical proce-dures with low to moderate bleeding risk,surgeons should be encouraged to operate on patients on DAPT.Adherence to DAPT should be improved through education of patients,relatives and physicians in order to prevent avoidable CV events.
5.2.6Duration of dual antiplatelet therapy
In patients with NSTE-ACS,DAPT with aspirin and clopidogrel has been recommended for 1year over aspirin alone,irrespective of re-vascularization strategy and stent type,according to the Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE)study,while the TRITON-TIMI 38and PLATO studies have demonstrated the superiority of a prasugrel-and ticagrelor-based regimen,re-spectively,over a clopidogrel-based one.138,148,153A 1-year duration of DAPT with clopidogrel was associated with a 26.9%RRR of death,MI or stroke (8.6%vs.11.8%;95%CI 3.9,44.4;P ?0.02)vs.1-month DAPT in the Clopidogrel for the Reduction of Events During Observation (CREDO)trial,which enrolled 2116pa-tients.183The study population comprised patients with stable CAD and low-risk NSTE-ACS undergoing PCI (each 50%),and no interaction between ACS status and DAPT was observed.
Evidence to support the extension of DAPT after DES beyond 1year in NSTE-ACS patients is limited (Table 9,see Web addenda).Table 9(see Web addenda)Main features of published randomized studies investigating various durations of dual antiplatelet therapy following percutaneous coronary intervention (PCI)
The DAPT trial randomized patients who did not experience ad-verse events in the ?rst year after PCI to an additional 18months of thienopyridine (clopidogrel/prasugrel)or placebo.184Continued treatment with thienopyridine,as compared with placebo,reduced the rates of stent thrombosis [0.4%vs.1.4%;HR 0.29(95%CI 0.17,0.48),P ,0.001]and major adverse cardiovascular and cerebrovas-cular events [4.3%vs.5.9%;HR 0.71(95%CI 0.59,0.85),P ,0.001].The rate of MI was lower with thienopyridine treatment than with placebo (2.1%vs.4.1%;HR 0.47,P ,0.001).The rate of death from any cause was 2.0%in the group that continued thienopyridine
ESC Guidelines
Page 19of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
therapy and 1.5%in the placebo group [HR 1.36(95%CI 1.00,1.85),P ?0.05].The rate of moderate or severe bleeding was increased with continued thienopyridine treatment [2.5%vs.1.6%;HR 1.61(95%CI 1.21,2.16),P ?0.001].184A meta-analysis including 32287patients enrolled in 10RCTs compared different DAPT durations.185Nearly 50%of the patients had stable CAD.Studies were strati?ed according to the DAPT duration in the control group in order to avoid having 12-month DAPT duration included in both study arms.As a consequence,it allowed comparison of outcomes of either short-term or extended (i.e.beyond 12months)DAPT duration vs.12-month https://www.doczj.com/doc/e314967604.html,pared with 12-month DAPT,a shorter course of treatment was associated with a signi?cant re-duction in major bleeds [OR 0.58(95%CI 0.36,0.92),P ?0.02],while no statistically signi?cant differences in ischaemic outcomes or stent thrombosis risks were observed,although a small to mod-erate increase could not be excluded.Extended DAPT,compared with 12-month treatment,yielded a signi?cant reduction in MI [OR 0.53(95%CI 0.42,0.66),P ,0.001]and stent thrombosis [OR 0.33(95%CI 0.21,0.51),P ,0.001]while more major bleeds occurred [OR 1.62(95%CI 1.26,2.09),P ,0.001].In addition,all-cause death was signi?cantly increased in the extended DAPT group [OR 1.30(95%CI 1.02,1.66),P ?0.03]while CV death did not dif-fer among the groups.185
The Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Back-ground of Aspirin-Thrombolysis in Myocardial Infarction 54(PEGASUS-TIMI 54)trial randomized 21162patients who had had an MI 1–3years earlier to ticagrelor at a dose of 90mg twice daily,ticagrelor at a dose of 60mg twice daily or placebo.186At a median follow-up of 33months,the study demonstrated a reduced rate of CV death,MI or stroke with ticagrelor [HR 0.85(95%CI 0.75,0.96),P ?0.008and HR 0.84(95%CI 0.74,0.95),P ?0.004for 90mg and 60mg of ticagrelor vs.placebo,respectively)and increased rates of major bleeding events (2.60%with 90mg,2.30%with 60mg and 1.06%with placebo,P ,0.001).186All-cause mortality did not differ between the groups.Of importance,most patients began treat-ment with ticagrelor after an interruption in DAPT and all had prior MI (context of secondary prevention in high-risk patients),while patients with a history of ischaemic stroke were excluded.In conclu-sion,while a 1-year duration of DAPT in NSTE-ACS patients is re-commended,based on individual patient ischaemic and bleeding risk pro?les,DAPT duration may be shortened (i.e.3–6months)or extended (i.e.up to 30months)in selected patients if required.5.2.7Glycoprotein IIb/IIIa inhibitors
Intravenous GPIIb/IIIa inhibitors block platelet aggregation by inhibiting ?brinogen binding to a conformationally activated form of the GPIIb/IIIa receptor on two adjacent platelets.128A meta-analysis of six RCTs involving 29570NSTE-ACS patients,mainly medically managed,showed a 9%RRR in death or non-fatal MI with GPIIb/IIIa inhibitors (10.7%vs.11.5%,P ?0.02)when added to heparin.196The greatest bene?t was observed in patients undergoing PCI while on these agents [10.5%vs.13.6%;OR 0.74(95%CI 0.57,0.96),P ?0.02].The use of GPIIb/IIIa inhibitors was associated with an increase in major bleeding complications without a signi?cant increase in intracranial haemorrhage.Many of these trials predated the routine use of P2Y 12inhibitors.While the relative ef?cacy of prasugrel and ticagrelor in the trials
appeared consistent among patients receiving and not receiving GPIIb/IIIa inhibitors,the ef?cacy and safety of GPIIb/IIIa inhibitors on top of these P2Y 12inhibitors have not been prospectively ad-dressed.153,197In patients treated with prasugrel or ticagrelor,GPIIb/IIIa inhibitors should be limited to bailout situations or thrombotic complications during PCI.Dosing in patients with impaired renal function is reported in Table 10.Additional informa-tion on GPIIb/IIIa inhibitors may be found in sections 5.2.7.1–5.2.7.3,while GPIIb/IIIa inhibitor-related thrombocytopenia is described in section 5.8.7.1(all in the Web addenda).5.2.7.1Upstream versus procedural initiation (see Web addenda)5.2.7.2Combination with P2Y 12inhibitors (see Web addenda)5.2.7.3Adjunctive anticoagulant therapy (see Web addenda)5.2.8Vorapaxar (see Web addenda)
5.2.9Recommendations for platelet inhibition in non-ST-elevation acute coronary syndromes
ESC Guidelines
Page 20of 59
by guest on November 11, 2015
https://www.doczj.com/doc/e314967604.html,/Downloaded from
2015 中国原发性肺癌诊疗规范 内容: 一、概述 二、病理诊断评估 三、分期 四、治疗 五、姑息治疗 (一)前言 原发性肺癌(以下简称肺癌)是我国最常见的恶性肿瘤之一。全国肿瘤登记中心2014年发布的数据显示,2010年,我国新发肺癌病例60.59万(男性41.63万,女性18.96万),居恶性肿瘤首位(男性首位,女性第2位),占恶性肿瘤新发病例的19.59%(男性23.03%,女性14.75%)。 肺癌发病率为35.23/10万(男性49.27/10万,女性21.66/10万)。同期,我国肺癌死亡人数为48.66万(男性33.68万,女性16.62万),占恶性肿瘤死因的24.87%(男性26.85%,女性21.32%)。肺癌死亡率为27.93/10万(男性39.79/10万,女性16.62/10万)。 在高危人群中开展肺癌筛查有益于早期发现早期肺癌,提高治愈率。低剂量 CT(low-dose computed tomography,LDCT)发现早期肺癌的敏感度是常规胸片的4-10 倍,可以早期检出早期周围型肺癌。国际早期肺癌行动计划数据显示,LDCT 年度筛查能发现85% 的I期周围型肺癌,术后10 年预期生存率达92%。 美国全国肺癌筛查试验证明,LDCT 筛查可降低20%的肺癌死亡率,是目前最有效的肺癌筛查工具。我国目前在少数地区开展的癌症筛查与早诊早治试点技术指南中推荐采用LDCT 对高危人群进行肺癌筛查。
美国国立综合癌症网络(National Comprehensive Cancer Network,NCCN)指南中提出的肺癌筛查风险评估因素包括吸烟史(现在和既往)、氡暴露史、职业史、患癌史、肺癌家族史、疾病史(慢阻肺或肺结核)、烟雾接触史(被动吸烟暴露)。 风险状态分3组:(1)高危组:年龄55-74 岁,吸烟史≥30包年,戒烟史<15 年(1 类);或年龄≥50 岁,吸烟史≥20包年,另外具有被动吸烟除外的项危险因素(2B 类)。(2) 中危组:年龄≥50 岁,吸烟史或被动吸烟接触史≥20包年,无其他危险因素。(3)低危组:年龄<50 岁,吸烟史<20包年。NCCN 指南建议高危组进行肺癌筛查,不建议低危组和中危组进行筛查。 为进一步规范我国肺癌的诊疗行为,提高医疗机构肺癌的诊疗水平,改善肺癌患者的预后,保障医疗质量和医疗安全,国家卫生和计划生育委员会医政医管局委托中国抗癌协会肿瘤临床化疗专业委员会,在原卫生部《原发性肺癌诊疗规范(2010 版)》的基础上进行了更新,制订了本规范。 (二)临床表现 1.肺癌早期可无明显症状,当病情发展到一定程度时,常出现以下症状:(1) 刺激性干咳。(2) 痰中带血或血痰。(3) 胸痛。(4) 发热。(5) 气促。当呼吸道症状超过2 周,经对症治疗不能缓解,尤其是痰中带血、刺激性干咳,或原有的呼吸道症状加重,要高度警惕肺癌存在的可能性。 2.当肺癌侵及周围组织或转移时,可出现如下症状: (1) 肿瘤侵犯喉返神经出现声音嘶哑。 (2) 肿瘤侵犯上腔静脉,出现面、颈部水肿等上腔静脉梗阻综合征表现。 (3) 肿瘤侵犯胸膜引起胸膜腔积液,往往为血性;大量积液可以引起气促。 (4) 肿瘤侵犯胸膜及胸壁,可以引起持续剧烈的胸痛。
银行营业部大堂经理简历 银行营业部大堂经理简历范文 姓名:吴好堤年龄: 22 户口所在:广州国籍:中国婚姻状况:未婚民族:汉族培训认证:未参加身高: 160 cm 诚信徽章:未申请体重: 43 kg 人才类型:在校学生应聘职位:营业部大堂经理:,人事专员:,文秘/文员:工作年限: 0 职称:无职称求职类型: 实习可到职日期:随时月薪要求: 1000--1500 希望工作地区:广州,, 工作经历 中国民生银行广州分行起止年月:xx-05 ~ xx-06 公司性质:股份制企业所属行业:银行担任职位:业务助理工作描述:1、寻找潜在客户。在中大轻纺城以陌生拜访的形式进行“乐收银”刷卡机的.市场推广工作,共售出20台刷卡机,排名第二。 2、跟单。把愿意使用“乐收银”刷卡机的客户带到民生银行越秀支行开户。 3、掌握“乐收银”刷卡机开户的手续程序。离职原因:实习结束广州市人力资源市场中心市场起止年月:xx-11 ~ xx-12 公司性质:事业单位所属行业:事业单位/社会团体担任职位:办公室助理工作描述: 1、主要负责“空岗审核”工作,日均拨打50个电话。 2、协助开展“岗前培训课程”,并指导受训人
员填写调查问卷。 3、运用办公软件文档资料。 4、清点资料、打印复印、制作证件等工作。离职原因:实习结束系青年志愿者协会起止年月:xx-10 ~ xx-06 公司性质:其它所属行业:其他行业担任职位:秘书部副部长工作描述: 1、撰写协会的计划总结书,多次主持例会,负责协会的财务管理工作。 2、作为负责人组织策划“广州市渔沙坦小学”心理咨询活动,坚持每周前往该校进行辅导工作。活动效果良好,获得校方好评。 3、以创新形式开展助学募捐活动,共筹得善款八千多元,全校排名第二。 4、积极参加协会的义工服务活动,例如到广州市盲人学校陪伴小朋友,前往康寿老人院看望老人,参加“四进社区”活动宣传广州亚运等。离职原因:学生干部换届 志愿者经历教育背景 毕业院校:广东金融学院最高学历:本科获得学位: 管理学位毕业日期: xx-06 专业一:劳动与社会保障专业二:起始年月终止年月学校(机构)所学专业获得证书证书编号语言能力 外语:英语一般粤语水平:优秀其它外语能力:国语水平:优秀工作能力及其他专长
2015年执业医师考试分数线公布 【天宇考王】为广大考生归纳总结执业医师最新考试资讯,让考生最先了解执业医师考试报名等有关事项的通知,避免错过报名失去考试机会,天宇考王是一款上机练习题库软件,有单机版、网页版、手机版、三位一体多平台学习模式。 各省、自治区、直辖市卫生计生委、中医(药)管理局、医师资格考试领导小组,国家医学考试中心、国家中医药管理局中医师资格认证中心: 经国家卫生计生委医师资格考试委员会2014年12月31日会议讨论决定,2014年医师资格考试医学综合笔试合格分数线为: 临床执业医师:363 临床执业助理医师:176 口腔执业医师:359 口腔执业助理医师:178 公共卫生执业医师:348 公共卫生执业助理医师:143 具有规定学历的中医执业医师:351 具有规定学历的中医执业助理医师:182 师承或确有专长中医执业医师:351 师承或确有专长中医执业助理医师:182 中西医结合执业医师:365 中西医结合执业助理医师:180 具有规定学历的蒙医执业医师:298 具有规定学历的蒙医执业助理医师:131 师承或确有专长蒙医执业医师:298 师承或确有专长蒙医执业助理医师:131 具有规定学历的藏医执业医师:346 具有规定学历的藏医执业助理医师:150
师承或确有专长藏医执业医师:346 师承或确有专长藏医执业助理医师:150 具有规定学历的维医执业医师:383 具有规定学历的维医执业助理医师:176 师承或确有专长维医执业医师:383 师承或确有专长维医执业助理医师:176 具有规定学历的哈萨克医执业医师:191 具有规定学历的哈萨克医执业助理医师:94 具有规定学历的中医(壮医)专业执业医师:272 具有规定学历的中医(壮医)专业执业助理医师:120 师承或确有专长中医(壮医)专业执业助理医师:120 更多考试最新资讯请点击天宇考王官网查看:https://www.doczj.com/doc/e314967604.html,
肿瘤科中医诊疗方案 肺癌诊疗方案 一、诊断 (一)疾病诊断 诊断标准:参照中华人民共和国卫生部医政司编《中国常见恶性肿瘤诊治规范·第六分册·原发性支气管肺癌》。 1.病理学诊断 无明显可确认之肺外原发癌灶,必须符合下列各项之一者,方能确立病理学诊断:(1)肺手术标本经病理、组织学证实者; (2)行开胸探查、肺针穿刺或经纤维支气管镜检采得肺或支气管活检组织标本,经组织学诊断为原发支气管肺癌者; (3)颈和腋下淋巴结、胸壁、胸膜或皮下结节等转移灶活检,组织学表现符合原发支气管肺癌,且肺或支气管壁内疑有肺癌存在,临床上又能排除其它器官原发癌者。 2.细胞学诊断 痰液、纤维支气管镜毛刷、抽吸、冲洗等细胞学标本,镜下所见符合肺癌细胞学标准者,诊断可以确立。需注意除外上呼吸道甚至食管癌肿。 3.符合下列各项之一者,可以确立临床诊断: (1)X线胸片见肺部有孤立性结节或肿块阴影,其边缘呈脑回状、分叶和细毛刺状,并在短期内(2-3个月)逐渐增大者,尤以经过短期积极药物治疗后可排除结核或其它炎性病变者; (2)节段性肺炎在短期内(一般为2-3个月)发展为肺不张,或肺叶不张在短期内发展为全肺不张者,或在其相应部位的肺根部出现肿块,特别是生长性肿块者; (3)上述肺部病灶伴远处转移,邻近器官受侵或压迫症状表现者,如:邻近骨破坏、肺门或/和纵隔淋巴结明显增大,短期内发展的上腔静脉压迫综合征、同侧喉返神经麻痹(排除结核和主动脉病变后)和颈部交感神经节(排除手术创伤后)、臂丛神经、膈神经侵犯症等。 肺癌的诊断多依据临床表现、影像学检查、病理学和细胞学检查以及血清学检查进行综合判断,其中病理学、细胞学检查结果是诊断肺癌的金标准。 (二)证候诊断 1.肺脾气虚证:久嗽痰稀、胸闷气短、神疲乏力、腹胀纳呆、浮肿便溏、舌质淡苔薄、边有齿痕、脉沉细。 2.肺阴虚证:咳嗽气短、干咳痰少、潮热盗汗、五心烦热、口干口渴、声音嘶哑、
2015年内科学综合测试题及答案1 选择一题 A1型 1.慢性支气管炎临床分型为: A.单纯型、混合型 B.单纯型、喘息型 C.急性型、慢性型、迁延型 D.单纯型、喘息型、迁延型 E.单纯型、喘息型、混合型 【答案】B 2.医院内获得性肺炎中,最常见的致病菌是 A.肺炎球菌 B.葡萄球菌 C.革兰氏阴性杆菌 D.厌氧菌 E.真菌 【答案】C 3.支气管哮喘中、重度发作首选药物 A.茶硷类 B.β受体激动剂 C.抗胆碱能类 D.糖皮质激素 E.抗过敏类 【答案】D 4.治疗高血压长期使用噻嗪类利尿剂可引起 A.低钾、低钠、高镁血症 B.低钙、低钠、低尿素血症
C.低钙、低钠、高尿素血症 D.高钾、低钠、低镁血症 E.低钾、低钠、低镁血症 【答案】E 5.下列各项检查中哪一项对诊断病毒性心肌炎意义较大 A.谷草转氨酶(SGOT) B.乳酸脱氢酶(LDH) C.红细胞沉降率(ESR) D.磷酸肌酸激酶(CPK) E.白细胞计数 【答案】D 6.慢性肺心病形成肺动脉高压的主要机制 A.支气管感染 B.红细胞增多 C.血液粘稠度增加 D.肺小动脉痉挛 E.肺毛细血管床减少 【答案】D 7.慢性胃炎的发病可能与那种细菌感染有关 A.大肠杆菌 B.沙门菌 C.幽门螺杆菌 D.空肠弯曲菌 E.嗜盐杆菌 【答案】C 8.左心功能不全最早期的体征为 A.舒张早期奔马律 B.交替脉
C.颈静脉怒张 D.肝肿大 E.下肢浮肿 【答案】A 9.最易发生幽门梗阻症状的溃疡是 A.胃角溃疡 B.胃窦溃疡 C.球后溃疡 D.幽门管溃疡 E.胃多发性溃疡 【答案】D 10.有高碳酸血症的慢性呼吸衰竭患者,适宜的吸氧浓度为 A.25%~30% B.35%~40% C.45%~50% D.55%~60% E.大于60% 【答案】A 11.下列哪一项是阿司匹林对冠心病心绞痛的治疗作用 A.降低血脂 B.消炎止痛 C.降低心肌耗氧量 D.抑制血小板聚集 E.抑制免疫反应 【答案】D 12.广泛心前壁梗塞是由于 A.左冠状动脉主干阻塞 B.左冠状动脉前降支阻塞
肺癌 【范围】 1.本指南规定了原发性肺癌(简称肺癌)的规范化诊治流程、诊断依据、诊断、鉴别诊断、治疗原则和治疗方案。 2.本指南适用于具备相应资质的市、县级常见肿瘤规范化诊疗试点医院及其医务人员对肺癌的诊断和治疗。 【术语和定义】 下列术语和定义适用于本指南。 (一)肺癌(lung cancer) 全称为原发性支气管肺癌,起源于支气管粘膜、腺体或肺泡上皮的肺部恶性肿瘤。 1.小细胞肺癌(small cell lung cancer,SCLC) 一种特殊病理学类型的肺癌,有明显的远处转移倾向,预后较差,但多数病人对放化疗敏感。 2.非小细胞肺癌(non-small cell lung cancer,NSCLC) 除小细胞肺癌以外其他病理学类型的肺癌,包括鳞状细胞癌、腺癌、大细胞癌等。在生物学行为和临床病程方面具有一定差异。 (二)中心型肺癌(central lung cancer) 生长在肺段支气管开口及以上的肺癌。 (三)周围型肺癌(peripheral lung cancer) 生长在肺段支气管开口以远的肺癌。 (四)隐性肺癌(occult lung cancer) 痰细胞学检查发现癌细胞,影像学和纤维支气管镜未发现病变的肺癌。 【缩略语】 下列缩略语适用于本指南。 1.CEA:(carcinoembryonic antigen) 癌胚抗原。 2.NSE:(neurone specific enolase)神经特异性烯醇化酶。 3.CYFRA21-1:(cytokeratin fragment)細胞角蛋白片段19。 【规范化诊治流程】
图1 肺癌规范化诊治流程 【诊断依据】 (一)高危人群 有吸烟史和/或肺癌高危职业接触史(如石棉),年龄在45岁以上者,是肺癌的高危人群。 (二)症状 1.肺癌早期可无明显症状,当病情发展到一定程度时,常出现以下症状:(1) 刺激性干咳。(2) 痰中带血或血痰。(3) 胸痛。(4) 发热。(5) 气促。当呼吸道症状超过2 周,经对症治疗不能缓解,尤其是痰中带血、刺激性干咳,或原有的呼吸道症状加重,要高度警惕肺癌存在的可能性。 2.当肺癌侵及周围组织或转移时,可出现如下症状: (1) 肿瘤侵犯喉返神经出现声音嘶哑。 (2) 肿瘤侵犯上腔静脉,出现面、颈部水肿等上腔静脉梗阻综合征表现。 (3) 肿瘤侵犯胸膜引起胸膜腔积液,往往为血性;大量积液可以引起气促。 (4) 肿瘤侵犯胸膜及胸壁,可以引起持续剧烈的胸痛。 (5) 上叶尖部肺癌可侵入和压迫位于胸廓入口的器官组织,如第一肋骨、锁骨下动、静脉、臂丛神经、颈交感神经等,产生剧烈胸痛,上肢静脉怒张、水肿、臂痛和上肢运动障碍,同侧上眼脸下垂、瞳孔缩小、眼球内陷、面部无汗等颈交感神经综合征表现。 (6) 近期出现的头痛、恶心、眩晕或视物不清等神经系统症状和体征应当考虑脑转移的可能。 (7) 持续固定部位的骨痛、血浆碱性磷酸酶或血钙升高应考虑骨转移的可能。 (8) 右上腹痛、肝肿大、碱性磷酸酶、天门冬氨酸氨基转移酶、乳酸脱氢酶或胆红素升高应考虑肝转移的可能。 (9) 皮下转移时可在皮下触及结节。
Superset的功能介绍 1、我们可以通过连接数据库,去对数据库中的单个表进行配置,展示出柱状 图,折线图,饼图,气泡图,词汇云,数字,环状层次图,有向图,蛇形图,地图,平行坐标,热力图,箱线图,树状图,热力图,水平图等图,官网上是不可以操作多个表的,不过我们可以操作视图,也就是说在数据库建好视图,也可以在superset中给表新增一列进行展示。 2、配置好了我们想要的图表之后我们可以把它添加到仪盘表进行展示,还可 以去配置缓存,来加速仪盘表的查询,不必要没次都去查询数据库。 3、我们可以查看进行查询表的sql,也可以把查询导出为json,csv文件。 它有自己的sql编辑器,我们可以在里面来编写sql。 一、系统基本使用 在使用本系统前,应该先进行账户的建立操作。 1.1登陆 输入开通的账号、密码点击登录即可。
1.2新建账号 在登陆时可以使用admin进行用户的创建。 先登陆admin用户,点击界面栏目"安全"→"用户列表"→,点击按钮 在填写完信息后点击保存(注:红色*的选项未必填项)即可使用新建账号登陆。
在创建账号时,根据使用账号功能需求选择不同的角色属性,每个账号的用户名不能相同。 二、创建数据源 2.1.1 superset连接MySQL 登录到部署superset主机 1.进入superset的Web界面,点击sources下拉选项的Databases,如下图: 2.进入数据库界面,点击“+”按钮进入数据库连接界面,填写正确字段后保存,操作如
下: 3.查看已经连接好的数据库 2.1.2 添加数据表 Sources -> T ables 点击加号(+)新增数据表 Database选择之前创建好的数据源,Table Name必须是数据源中对应真实的表名,表中必须包含一个Date或者Timestamp类型的字段
JBKL型燃烧器PVC全自动 操作手册 大庆国科盛鑫节能环保设备制造有限公司 前言 我国是全世界自然资源浪费最严重的国家之一,在59个接受调查的国家中排名第56位。另据统计,中国的能源使用效率仅为美国的26.9%,日本的11.5%。为此,近年来我国推行了多项节能减排政策措施。目前,为了实现“十一五”规划中确定的单位GDP能耗降低20%的目标、主要污染物排放总量减少10%的约束性指标,国务院发布了继续加强节能工作的决定,节能减排工作迫在眉睫。 在举国重视节能减排工作的大形势下,我公司自主创新,目前已经自主研发9项国家专利技术,全部是节能减排燃油燃气燃烧器技术。我公司发展势头强劲,不断创新探索,为全国节能减排事业做出自己应有的责任。 我公司研发节能减排燃烧器过程中发现,目前小型取暖锅炉普遍使用的国内外燃烧器采用的程序控制工艺是:锅炉出口水温度到达给定值上限后,电磁阀关闭,炉灭火。锅炉出口水温度降到下限时锅炉重新启动,送风机进行3-5分钟炉膛扫线,这时大量冷风进入炉膛里,把炉膛温度大幅降下来,扫完炉膛后,重新喷燃气点火升温,这样消耗燃气量增加。因此我公司燃烧器程序控制是采用自动调节阀来控制燃气喷大小量,锅炉出口水
温平稳,安全运行,提高节能减排数据。 JBKL型燃气燃烧器的设计说明 JBKL型燃烧器主要是针对目前燃气燃烧器喷咀存在的问题而设计的。存在的问题是: 1、目前国内外使用的燃气喷咀是直线喷燃气方式,国际上燃烧器技术较发达的意大利、法国、德国等国家的相关技术也是直线喷燃气方式。燃气是靠自身压力通过燃气喷咀直线喷入炉膛里的,燃气压力而产生的冲力使燃气与空气在推进的一段距离内不容易混合好,因此燃气在逐步扩散中与空气边混合边燃烧,这样炉膛内的火型长,高温度热量停留在炉膛内的受热时间短,使排烟温度升高,导致热效率降低。当加负荷增加燃气压力时冲力增大,烟气在炉膛内的流速加快,排烟温度迅速升高,热效率更低。 2、目前油田加热炉、炼油厂加热炉使用的配风器都是配直流风方式,直流风和燃气混合时出现各走各的现象,完全燃烧所需要的时间长,需要大量的配风才能满足燃烧,在运行时高温度烟气向前的推动力很大,当加负荷加大配风量时,推动力更大,这是加热炉热效率低的重要因素。 针对这样的问题,我们紧紧抓住安全运行、稳定燃烧、快速完全燃烧、配备最佳空气、控制最佳烟气流速和提高炉热效率的关键因素,对锅炉燃烧器相关的结构和部位进行研究和开发,并采取了以下几点措施: 1、燃气压力设计在燃气喷枪管内,运行时燃气冲力产生真空度,利用这个动力把空气吸进来,燃气和空气提前有效地混合,缩短了燃烧的过程和时间,喷出的混合气体立即迅速燃烧,高温度的能量停留在炉膛内的时间长,排烟温度低,提高热效率。
乐收银产品介绍 【产品介绍】 乐收银是我行专门针对批发市场客户研发的电话POS,T+0 入 账,接受所有银行借记卡刷卡,享受批发扣率,贡献度高的可享受优惠费率。 【产品定义】 乐收银是我行专为批发贸易类小微企业定制的新型支付结算服 务产品,支持使用个人借记卡,集合了传统POS 和第三方电话支付终端产品的优点,集刷卡收款、转账付款、账户查询等功能于一身,能有效提高商户结算效率,降低商户结算成本。 【乐收银的适用对象】 优先选择江苏银联认定的批发大市场名单内商户,尤其是满足我 行开立商户卡客户;其次,按照相关要求,乐收银终端应严格限制于无集中收银的批发市场批发商户范围内使用。 批发市场内的商户需满足以下任一条件: 1、经营门店在专业批发市场内; 2、商户实际经营门店地址与营业执照注册地址不一致的,需商 户单独开具证明; 3、营业执照注册地址未注明在批发市场内的,但实际经营门店 地址在批发市场内的,需出具在市场内的摊位租赁合同复印件、产权证明复印件或市场管理方出具的相关证明,并加盖公章。 【乐收银的主要特色】
产品主要特色如下: 1、借记卡刷卡收款T+0 实时到账,可以做到实时收款、实时到账、实时可用,从而提高资金利用效率。 2、手续费上可以封顶,商户卡尽享优惠,节约财务费用成本, 满足我行特定标准可享受刷卡手续费优惠政策,最高可以全免; 手续费标准 收单银行受理卡种收款费率汇款费率 民生银行 本行卡免费 1.商户卡、银卡每日累计汇款金额 分别50 万(含)以下免费,超部 分按照普通卡标准; 2.金卡每日累计汇款100 万以下 免费,超出部分按照普通卡标准; 3.钻石卡免费。 他行卡 0.78%—26 元封顶 (达到考核标准免费) 3、终端自助转账、还款足不出户,实时到账,节省宝贵时间, 手续费更优惠; 4、根据刷卡交易流水,可获得信用贷款,免抵押担保; 5、余额查询:终端上可自主查询卡内余额,实时掌控资金储备。【如何办理】 1、商户资料准备。申请安装乐收银商户需填写《中国民生银行 乐收银商户业务开通申请表》、《中国民生银行特约商户信息调查表》,并提供以下材料: ①营业执照、税务登记证、法人代表或负责人身份证,以上材料 需核对原件,留存复印件1 份;如商户负责人授权委托受托人开立民生借记卡,并将其作为交易资金的入账账户的,除提供法人代表或负
2015年肺癌诊疗指南:共识和争议 原发性肺癌(以下简称肺癌)是我国最常见的恶性肿瘤之一。最新的卫生统计年鉴显示,肺癌死亡率占我国恶性肿瘤死亡率的第一位。目前常用的肺癌临床诊疗指南包括:美国临床肿瘤学会(ASCO)肺癌诊疗指南、美国国家综合癌症网(NCCN)肺癌诊疗指南、欧洲肿瘤内科学会(ESMO)肺癌诊疗指南以及中国卫生部(现国家卫生计生委)原发性肺癌诊疗规范。各个指南在总体原则上并无明显差异,但在具体的处理细节上有所区别。本文将结合最新的诊疗指南,介绍肺癌临床研究的共识与争议,并通过相关的临床证据进行解读。 早期非小细胞肺癌(Ⅰ期、Ⅱ期) 共识一:对于早期肺癌,肺叶切除,纵隔淋巴结清扫以期实现R0 切除是首选的治疗方式。在尽可能实现R0 切除的前提下,施行电视辅助胸腔镜(VATS)肺叶切除术也是可行的。 争议一:NCCN 指南认为,除行纵隔淋巴结清扫外,可进行系统淋巴结采样;IASLC 则具体规定最少清扫6 组淋巴结,其中3 站必须是纵隔淋巴结包括隆突下淋巴结。 如何在完整切除肿瘤病灶的前提下,最大限度地保存患者的正常肺组织,减少手术创伤是我们的目标,尤其对于肺功能差的患者具有更大的现实
意义。由此提出了亚肺叶切除的概念,包括解剖性肺段切除和肺楔形切。早期研究显示与肺叶切除相比,肺段切除和楔形切除显著增加局部复发的风险,因此肺叶切除仍是当前标准切除方式。但由于CT 筛查技术的运用,更多的小结节磨玻璃样(GGO)病灶被发现,最近大样本的回顾性研究显示:Ⅰ期患者亚肺叶切除vs. 肺叶切除的荟萃分析:14 项研究(12 项回顾性研究;1 项配对研究;1 项随机研究);903 例亚肺叶切除患者;1887 例肺叶切除患者。1 年、3 年和5 年生存率差别分别为0.7%、1.9% 和3.6%,虽然这些差异显示亚肺叶切除更优,但均无统计学意义。以上回顾性研究结果提示我们经过严格的选择符合以下标准的手术人群是可以考虑接受亚肺叶切除的,如仅为ⅠA 期,直径不超过2——3cm 的小肿瘤,周围肺肿瘤(可以扩大切除边缘),CT 图像表现为以GGO 为主。但若要评价在早期的ⅠA 期患者中亚肺叶切除是否具有相对于传统肺叶切除的更大的优势?目前还缺乏确切的前瞻性随机对照临床研究数据,而正在进行的亚肺叶切除的临床试验CALBG 140503 和JCOG0802/WJOG4607L或许能帮助我们回答这一问题。 共识二:对于不能耐受手术的患者,包括我国指南在内的几大治疗指南也都推荐进行放疗,尤其是将立体定向放疗(SABR)作为根治Ⅰ期肺癌的可行手段。 争议二:对于术后辅助放疗的适用人群目前还存在争议:ESMO 指南推荐:肿瘤直径>5cm 和(或)中央型肺癌,推荐进行常规放疗或者加速
优秀个人简历范文文章3篇 姓名:某某某 性别:男 出生年月:1985年10月8日 居住地:西安 电话:XXXXXXXXXXX 求职意向 到岗时间:一周以内 工作性质:全职 希望行业:金融/投资/证券 目标地点:西安 期望月薪:面议/月 目标职能:证券分析师 工作经验 2021 /1—至今:XX金融证券有限公司 所属行业:金融/投资/证券 研发部证券分析师 1、负责通过股市报告会、面谈等形式,营销理财服务; 2、负责分析目标板块的上市公司的基本面,列出投资原因,并给出风险提示; 3、负责宏观经济、政策走向分析及解读; 4、负责协助基金经理,对持仓比重、结构、品种做出建议; 5、负责协助其他分析师进行投资组合的配置。 2021/10--2021 /12:XX金融证券有限公司 所属行业:金融/投资/证券
市场部证券分析师 1、负责为客户提供投资理财咨询; 2、负责组建及管理投资顾问团队,维护投资渠道; 3、负责维护客户关系,推广并销售公司的金融理财产品; 4、负责通过数据、技术面的分析来进行股票买卖的实盘操作; 5、负责定期召开投资报告会,培训客户经理的投资分析知识。 2021 /11--2021/7:XX金融有限公司 所属行业:金融/投资/证券 投资部证券分析师 1、负责研究中国宏观经济、市场状况和投资环境,分析投资行业政策、产业政策以及公司的经营情况; 2、负责跟踪****行业动态,并对行业内变化个股做出分析评价; 3、负责维护客户,为客户提供咨询服务; 4、负责***基金的交易,并指导交易员完成交易指令; 5、负责培训下属员工以及分配部门任务。 教育经历 2021/9 --2021 /7 西安理工大学金融学本科 语言能力 英语良好听说熟练,读写良好 自我评价 在证券公司任职***年,对于股票投资具有深入的研究,善于数据挖掘和财务分析,对于国家政策和经济形势发展具有敏锐的观察力。具有出色的逻辑思维能力和写作能力,曾在知名财经杂志发表文章数篇,得到读者的欢迎。能够承受巨大的工作强度,抗压能力强,工作责任心高,团队合作意识佳,希望在证券行业继续发展。 姓名:xxx 性别:男
百度外卖产品操作操作流程 接单: 1:平台会提前一小时下单,(前期是电话下单,后期会接入点餐系统)门店在接单后制作产品,对产品按计量包装好后放入制定位置,平台骑手会在规定的时间进行取餐 2:后厨在接单后15分钟内必须出完所有产品,打包好后装入食品袋放入门店指定的位置。 产品范围: 6种锅底:菌王糊辣鸳鸯锅、菌王柠檬鸳鸯锅、菌王酸汤鸳鸯锅、菌王鲜辣鸳鸯锅、菌王养颜木瓜鸳鸯锅、菌王滋补鸳鸯锅、菜单上除果汁与果酒所有产品。产品标准: 菌王糊辣鸳鸯锅 1:配制好的成品菌汤,包装规格900克/袋,(含香菇片,鸡油,配制标准同现有的菌汤标准) 2:糊辣底料一袋,包装规格900克/袋(含配糊辣锅的辅料,如子弹头,灯笼椒,醪糟,冰糖等,搅拌均匀装袋,标准和现有的标准一样)
菌王柠檬鸳鸯锅 1:配制好的成品菌汤,包装规格900克/袋,(含香菇片,鸡油,配制标准同现有的菌汤标准) 2:柠檬底料一袋,包装规格900克/袋,(含香茅草、柠檬叶、鲜红小米辣、搅拌均匀装袋、配制标准同现有的柠檬锅底标准) 菌王酸汤鸳鸯锅 1:配制好的成品菌汤,包装规格900克/袋,(含香菇片,鸡油,配制标准同现有的菌汤标准) 2:配制成品酸汤900克(含香茅草、木姜子油、番茄片、香菜段,搅拌均匀装袋、配制标准同现有的酸汤锅底标准) 菌王鲜辣鸳鸯锅 1:配制好的成品菌汤,包装规格900克/袋,(含香菇片,鸡油,配制标准同
现有的菌汤标准) 2:鲜辣底料一袋,包装规格900克/袋(含鲜辣底料,高汤,泡小米辣,姜片,大葱,搅拌均匀装袋、标准和现有的鲜辣锅底标准一样) 菌王金汤鸳鸯锅 1:配制好的成品菌汤包装规格900克/袋,(含香菇片,鸡油,配制标准同现有的菌汤标准) 2:金汤锅底一袋,包装规格900克/袋(含,金汤底料,木瓜,枸杞,党参,当归,大枣,搅拌均匀装袋,标准和现有的金汤锅底标准一样) 菌王滋补鸳鸯锅 1:配制好的成品菌汤,包装规格900克/袋,(含香菇片,鸡油,配制标准同现有的菌汤标准) 2:配制好的成品滋补汤,包装规格900克/袋,(姜片,大枣,枸杞,鸡油,配制标准同现有的滋补锅标准一样) 打包器皿:
2015年执业医师考试报名条件最新消息 【天宇考王】为广大考生归纳总结执业医师最新考试资讯,让考生最先了解执业医师考试报名等有关事项的通知,避免错过报名失去考试机会,天宇考王是一款上机练习题库软件,有单机版、网页版、手机版、三位一体多平台学习模式。 《中华人民共和国执业医师法》相关规定,内容如下: 第九条具有下列条件之一的,可以参加执业医师资格考试: (一)具有高等学校医学专业本科以上学历,在执业医师指导下,在医疗、预防、保健机构中试用期满一年的; (二)取得执业助理医师执业证书后,具有高等学校医学专科学历,在医疗、预防、保健机构中工作满二年;取得执业助理医师执业证书后,具有中等专业学校医学专业学历,在医疗、预防、保健机构中工作满五年的。注:台湾、香港、澳门居民报考医师资格考试,请参阅《关于取得内地医学专业学历的台湾香港澳门居民申请参加国家医师资格考试有关问题的通知》。 《医师资格考试报名资格规定(2014版)》自2014年3月18日公布施行,依据此规定“学历审核”内容如下: 学历的有效证明是指国家承认的毕业证书。基础医学类、法医学类、护理(学)类、医学技术类、药学类、中药学类等医学相关专业,其学历不作为报考医师资格的学历依据。 (一)研究生学历 1.临床医学专业学位研究生,在符合条件的医疗、预防、保健机构进行临床实践,至当次医学综合笔试时累计实践时间满1年的,以符合条件的本科学历和专业,于在学期间报考临床类别医师资格。临床医学、眼视光医学长学制学生在学期间已完成1年临床毕业实习和1年以上临床实践的,以本科学历报考临床类别医师资格。 2.临床医学专业学位研究生学历,作为报考临床类别医师资格的学历依手机版、网页版、单机版三位一体多平台学习模式据。在研究生毕业当年以研究生学历报考者,须在当年8月31日前提交研究生毕业证书,并提供学位证书等材料,证明是专业学位研究生学历,方可参加医学综合笔试。 3.2014年12月31日以前入学的临床医学专业的学术学位(原“科学学位”)研究生,具有相当于大学本科1年的临床毕业实习和1年以上的临床实践的,该研究生学历和学科作为报考临床类别医师资格的依据。在研究生毕业当年报考者,须在当年8月31日前提交研究生毕业证书,方可参加医学综合笔试。 2015年1月1日以后入学的学术学位研究生,其研究生学历不作为报考各类别医师资格的学历依据。 4.临床医学(护理学)学术学位研究生学历,或临床医学(护理领域)专业学
第二篇服务我专业 第2.1问乐收银常用功能菜单是哪些 1.签到 操作步骤: (1)选择“签到”菜单,按“确认”键; (2)机具提示签到成功。 2.余额查询 操作步骤: (1)选择“余额查询”; (2)以刷卡方式输入卡号; (3)通过密码键盘输入正确的交易密码 (4)机具返回卡可用余额。 3.老板收款 操作步骤: (1)选择“老板收款”;以刷卡方式输入卡号; (2)输入消费金额; (3)通过密码键盘输入正确的交易密码; (4)交易成功并打印凭条,为了出现差错时便于银行调单,建议您打印3联交易凭证。 4.付款 操作步骤: (1)选择“付款”功能; (2)选择汇款方式,支持3类汇款方式:“行内汇款”、“普通跨行汇款”、“快速跨行汇款”; (3)汇款方式选择完成后,根据提示,输入两次汇入账号,也可刷卡输入,前后两次输入的汇入账号必须一致,按确认键; (4)输入付款金额,按确认键;
(5)提示“汇出账号”,以刷卡的方式输入卡号,按确认键; (6)通过密码键盘输入正确的交易密码,按确认键,提交交易请求; (7)交易成功并打印凭条。 5.交易统计 操作步骤: (1)选择“交易统计”功能; (2)输入需要统计的日期; (3)机具返回消费笔数合计、消费金额合计、入账笔数合计、入账金额合计、付款笔数合计、付款金额合计,按0键往下换页。 乐收银机具常用功能菜单列表 一级菜单二级菜单三级菜单 1、银联服务 1.1签到 1.2余额查询 1.3收款 1.4付款 1.4.1行内汇款 1.4.2普通跨行汇款 1.4.3快速跨行汇款1.5交易统计 1.6在线账单 1.6.1未支付 1.6.2已支付账单 1.6.3收取账单 1.6.4短信收件箱 2、短信账单 3、通话记录 4、终端更新 5、个人助理 6、设置6.1基本设置 6.1.1时间设置 6.1.2液晶对比度设置 6.1.3背光设置 6.1.4交易提示音开关6.2高级设置 6.2.1预设外线号码 6.2.2来电自动应答
产品部产品上线操作流程及规范 一、编写本流程和规范目的 为提升平台的整体形象以及消费者的用户体验,提升平台竞争力,便于产品部对产品上架操作的规范化、正规化,明晰与供应商的合作流程及规范,特制定此流程及规范。 二、本标准的适用范围 本流程及规范适用于产品部在主动选择或筛选供应商提供的产品是否符合平台要求,以及产品部在与意向供应商接洽时的具体操作内容方面。在产品的初选、评估到最后上线均适用与本流程及规范。 三、术语与定义(无) 四、招商工作中的内容与规定 1.招商工作流程
2.在平台上线产品必须为平台可经营的产品 平台可经营种类为:农副产品、水果、预包装食品、进口酒类、国产酒类、非酒精饮料及茶叶、电子产品、日用百货的销售、礼品鲜花、小饰物、小礼品。平台销售的产品主要为农副产品、水果、预包装食品及中高端生活类用品。尤其以绿色生态农产品及其加工制品为主要发展方向。 3.供应商资质必须符合平台的标准 主体:与四翁合作主体必须为国家法律承认的企业法人或其自然人代表。生产企业名优企业优先。 资质:与四翁合作主体需向四翁提交营业执照、税务登记证(地税、国税)、商标注册证、组织机构代码证及其它必须的相关许可。 产品:产品有较强的市场卖点及售价优势,适合于互联网销售及物流运输。并提供产品的宣传图样若干,及产品详细信息(类似于淘宝及京东商城样式)。 五、职责与权限 1.商品上线前供应商需提供的资料及其他相关事宜 1.1 供应商需提供给平台需上线的产品图片,具体要求如下:600*600Px 主图1-3张(高清无码,无不相关水印、logo),产品详情图3-6张(无不相关水印、logo,宽与高500px*1500px,像素达到72的宝贝描述详情图),必须与所销售产品实物相吻合且附带产品介绍的文字资料。所有图片必须为高清图片,创意艺术拍摄并精修,图片明亮美观,能激起顾客的购买欲望,手机拍摄像、未处理照片不予采纳。 1.2 产品详情图中需包含产品的产地、主要成分、产品规格、产品保质期、使用说明及禁忌。图片清晰美观,布局合理。 1.3 为保证平台的美观及整体档次,平台有权利对产品形象不合格的产品予以下架或不上架处理。供应商无法提供合格图片的,可委托平台协助拍摄处理产品图片,费用由供应商承担。 1.4 产品包装符合物流运输要求,安全性强,稳定性高,避免运输过程中发生损坏。 1.5 产品上架前,供货商需向平台提供不少于2个购买单位的商品体验装,以便于平台了解体验此产品。体验装必须与供货商所提供给平台销售的
2015年全国执业医师考试报考条件 2014年执业医师考试真题、模拟题尽收其中,千名业界权威名师精心解析,精细化试题分析、完美解析一网尽!在线做题就选针题库:https://www.doczj.com/doc/e314967604.html,/oXVZF 全国2015年执业医师报名条件 根据《中华人民共和国执业医师法》及有关规定具有下列条件之一的,可以参加医师资格考试: (一)具有高等学校医学专业本科以上学历,在执业医师指导下,在医疗、预防、保健机构中试用期满一年的; (二)取得执业助理医师执业证书后,具有高等学校医学专科学历,在医疗、预防、保健机构中工作满二年;具有中等专业学校医学专业学历,在医疗、预防、保健机构中工作满五年的。 (三)具有高等学校医学专科学历或者中等专业学校医学专业学历,在执业医师指导下,在医疗、预防、保健机构中试用期满一年的,可以参加执业助理医师资格考试。 以师承方式学习传统医学满三年或者经多年实践医术确有专长的,经县级以上人民政府卫生行政部门确定的传统医学专业组织或者医疗、预防、保健机构考核合格并推荐,可以参加执业医师资格或者执业助理医师资格考试。考试的内容和办法由国务院卫生行政部门另行制定。 (四)符合《医师资格考试报名资格规定(2006) 》。 注:台湾、香港、澳门居民报考医师资格考试,请参阅《关于取得内地医学专业学历的台湾香港澳门居民申请参加国家医师资格考试有关问题的通知》。 口腔执业医师报考指南 考试介绍 医师资格考试的性质是行业准入考试,是评价申请医师资格者是否具备从事医师工作所必须的专业知识与技能的考试。口腔执业医师考试分实践技能考试和医学综合笔试两部分。 口腔执业医师实践技能考试采用三站式考试的方式。考区、考点按照《医师资格实践技能考试实施方案》的要求设立实践技能考试基地,考生在实践技能考试基地依次通过“三站”接受实践技能的测试。每位考生必须在同一考试基地内完成全部考站的测试。 口腔执业医师医学综合笔试考试于9月中旬举行,具体时间以国家卫生和计划生育委员会医师资格考试委员会公告时间为准。口腔执业医师考试时间为2天,分4个单元,每单元均为两个半小时。
2017版CSCO肺癌指南 2017 年4 月22 日,中国临床肿瘤学会(CSCO)指南发布会在广州举行。CSCO 副理事长、吉林省肿瘤医院院长程颖教授就《CSCO 原发性肺癌诊疗指南》2017 年更新版进行了解读。 那么,2017 版《CSCO 原发性肺癌诊疗指南》中究竟更新了哪些内容?又是基于哪些证据呢?让我们一起来看一下。 在影像和分期诊断部分、病理学诊断部分以及随访部分,内容没有变化。 分子分型部分的更新 在基本策略中,非鳞癌除了EGFR 和ALK 融合基因检测外,新增加了耐药后行二次活检对继发耐药T790M 进行检测,不能行组织学检测的患者可行血液ctDNA T790M 检测(I 类证据)。 可选策略中,增加了ROS1 融合基因RT-PCR 检测(从IIA 类提到IB 证据)。更新ROS1 检测方法,主要是基于
吴一龙教授牵头的东亚ROS1 阳性患者的II 期研究,入组127 例病人,其中中国患者74 例,使用RT-PCR 方法,阳性患者使用克唑替尼治疗。其中CR 14 例,PR 74 例,ORR 69.3%,PFS 13.4 个月,ROS1 成为克唑替尼治疗有效的第二个分子类型。 基于病理类型,分期和分子分型的综合治疗部分的更新 1. 非小细胞肺癌(NSCLC)治疗的更新 (1)不可手术的IIIA 或IIIB 期NSCLC PS 0-1 者新增加了同步放化疗证据。证据来自于王绿化教授的III 期研究,比较依托泊甙/ 顺铂和紫杉醇/ 卡铂同步放化疗随机对照研究,3 年OS 率分别是41.4% 和26.0%,因此推荐依托泊甙/ 顺铂为IIIA 或IIIB 期不能手术患者的优选同步放化疗方案。 (2)IV 期EGFR 突变患者的一线治疗 PS 0-3 分者,按照上市时间,在基本策略里推荐吉非替尼,埃克替尼,厄洛替尼和阿法替尼,其中阿法替尼是今年增加的证据。可选策略里,PS 0-1 分者增加了联合化疗循证医学依据。此推荐基于JMIT 研究,EGFR 突变患者使用
卫生部肺癌诊疗指南(2011) 一、概述 原发性肺癌(以下简称肺癌)是我国最常见的恶性肿瘤之一。2010年卫生统计年鉴显示,2005年,肺癌死亡率占我国恶性肿瘤死亡率的第1位。 为进一步规范我国肺癌诊疗行为,提高医疗机构肺癌诊疗水平,改善肺癌患者预后,保障医疗质量和医疗安全,特制定本规范。 二、诊断技术与应用 (一)高危因素。有吸烟史并且吸烟指数大于400支/年、高危职业接触史(如接触石棉)以及肺癌家族史等,年龄在45岁以上者,是肺癌的高危人群。(二)临床表现。 1.肺癌早期可无明显症状。当病情发展到一定程度时,常出现以下症状:(1)刺激性干咳。 (2)痰中带血或血痰。 (3)胸痛。 (4)发热。 (5)气促。 当呼吸道症状超过两周,经治疗不能缓解,尤其是痰中带血、刺激性干咳,或原有的呼吸道症状加重,要高度警惕肺癌存在的可能性。 2.当肺癌侵及周围组织或转移时,可出现如下症状: (1)癌肿侵犯喉返神经出现声音嘶哑。 (2)癌肿侵犯上腔静脉,出现面、颈部水肿等上腔静脉梗阻综合征表现。(3)癌肿侵犯胸膜引起胸膜腔积液,往往为血性;大量积液可以引起气促。(4)癌肿侵犯胸膜及胸壁,可以引起持续剧烈的胸痛。
(5)上叶尖部肺癌可侵入和压迫位于胸廓入口的器官组织,如第一肋骨、锁骨下动、静脉、臂丛神经、颈交感神经等,产生剧烈胸痛,上肢静脉怒张、水肿、臂痛和上肢运动障碍,同侧上眼脸下垂、瞳孔缩小、眼球内陷、面部无汗等颈交感神经综合征表现。 (6)近期出现的头痛、恶心、眩晕或视物不清等神经系统症状和体征应当考虑脑转移的可能。 (7)持续固定部位的骨痛、血浆碱性磷酸酶或血钙升高应当考虑骨转移的可能。(8)右上腹痛、肝肿大、碱性磷酸酶、谷草转氨酶、乳酸脱氢酶或胆红素升高应当考虑肝转移的可能。 (9)皮下转移时可在皮下触及结节。 (10)血行转移到其他器官可出现转移器官的相应症状。 (三)体格检查。 1.多数肺癌患者无明显相关阳性体征。 2.患者出现原因不明,久治不愈的肺外征象,如杵状指(趾)、非游走性肺性关节疼痛、男性乳腺增生、皮肤黝黑或皮肌炎、共济失调、静脉炎等。 3.临床表现高度可疑肺癌的患者,体检发现声带麻痹、上腔静脉梗阻综合征、H orner征、Pancoast综合征等提示局部侵犯及转移的可能。 4.临床表现高度可疑肺癌的患者,体检发现肝肿大伴有结节、皮下结节、锁骨上窝淋巴结肿大等提示远处转移的可能。 (四) 影像检查。 1.胸部X线检查:胸片是早期发现肺癌的一个重要手段,也是术后随访的方法之一。
2015年临床执业医师考试历年真题及解析 2015年临床执业医师考试真题、模拟题尽收其中,千名业界权威名师精心解析,精细化试题分析、完美解析一网尽!在线做题就选针题库:https://www.doczj.com/doc/e314967604.html,/oXVZF 一、以下每一道题下面有A、B、C、D、E五个备选答案。请从中选择一个最佳答案,并在答题卡上将相应题号的相应字母所属的方框涂黑。 1.★★★下列哪项符合门脉性肝硬化的典型病理变化 A.广泛的肝细胞变性坏死 B.正常肝小叶结构破坏 C.结缔组织增生 D.肝内血管网改建 E.再生结节及假小叶形成 正确答案:E 题解:早期肝体积正常或略增大,质地稍硬。后期肝体积缩小,重量减轻表现呈结节状,结节大小相仿,最大结节直径不超1.0cm。切面结节间为纤维组织间隔,间隔宽窄一致。镜下正常小叶结构被破坏,由假小叶取代,假小叶是由广泛增生的纤维组织将肝细胞再生结节分割包绕成大小不等、圆形或椭圆形的肝细胞团。假小叶内肝细胞索排列紊乱,肝细胞再生明显,小叶中央静脉缺如、偏位或有两个以上,假小叶外可见慢性炎细胞浸润,小胆管常有增生和淤胆,可见肝细胞的变性坏死。 2.★★★急性炎症早期局部浸润的炎细胞主要是 A.嗜中性粒细胞 B.嗜酸性粒细胞 C.嗜碱性粒细胞 D.浆细胞 E.淋巴细胞 正确答案:A
题解:炎症区血管内的液体和细胞成分通过血管壁进入组织间隙、体腔或体表、黏膜表面的过程称渗出,渗出的液体和细胞成分称为渗出物。渗出的细胞中中性粒细胞运动活跃、吞噬功能强、可释放内源性致热原。主要见于急性炎症的早期,特别是化脓性炎症;单核细胞及巨噬细胞运动及吞噬能力强,可发挥免疫效应,释放内源性致热原,主要见于急性炎症后期、慢性炎症以及病毒、寄生虫感染时;嗜酸性粒细胞能吞噬抗原-抗体复合物,主要见于免疫异常疾病,寄生虫的感染及急性炎症后期;T细胞参与细胞免疫,B 细胞在抗原刺激下转变为浆细胞,产生抗体参与体液免疫过程,主要见于慢性炎症和病毒感染性疾病。 3.★★★不属于凝固性坏死的病变是 A.肝阿米巴脓肿 B.心肌梗死 C.干酪样坏死 D.肾梗死 E.肝细胞嗜酸性小体 正确答案:A 题解:凝固性坏死是指坏死组织由于失水变干,蛋白质凝固而变成灰白或黄白色比较坚实的凝固体,故称为凝固性坏死。常见于脾、肾的贫血性梗死,镜下特点为坏死组织的细胞结构消失,但组织结构的轮廓依然保存。其包含几种特殊类型:干酪样坏死和坏疽。 4.★★★急性病毒性肝炎(普通型)的病变特点是肝细胞 A.广泛变性,坏死轻微 B.广泛坏死,变性轻微 C.广泛再生,变性较轻 D.广泛坏死,再生较轻 E.变性、坏死、再生均广泛 正确答案:A 题解:急性普通型肝炎的病理特点为肝细胞广泛变性而坏死轻,变性多为气球样变,坏死多为点状坏死。 5.★★★关于玻璃样变性,下述哪项是错误的 A.可发生于结缔组织 B.可发生于血管壁 C.可发生于浆细胞