Therapeutic Drug Monitoring
Issue: Volume 20(6), December 1998, pp 612-618
Copyright: ? 1998 Lippincott Williams & Wilkins, Inc.
Publication Type: [Articles]
ISSN: 0163-4356
Accession: 00007691-199812000-00005
Keywords: Population pharmacokinetics, Vancomycin, Pediatric patients, Methicillin-resistant Staphylococcus aureus (MRSA), NONMEM, Dosage guideline
[Articles]
Population Pharmacokinetics of Vancomycin in Japanese Pediatric Patients
Yasuhara, Masato*; Iga, Tatsuji?; Zenda, Hiroshi?; Okumura, Katsuhiko§; Oguma, Takayoshi[//]; Yano, Yoshitaka[//]; Hori, Ryohei?
Author Information
*Department of Pharmacy, Tokyo Medical and Dental University Hospital, Tokyo; ?Department of Pharmacy, Tokyo University Hospital, Tokyo; ?Department of Pharmacy, Shinshu University Hospital, Matsumoto; §Department of Pharmacy, Kobe University
Hospital, Kobe; [//]Developmental Research Laboratories, Shionogi and Co., Ltd., Osaka; and ?Pharmaceutical Research and Technology Institute, Kinki University, Osaka, Japan.
Received December 11, 1997; accepted June 24, 1998.
Address correspondence and reprint requests to Takayoshi Oguma, Developmental Research Laboratories, Shionogi and Co., Ltd., Sagisu 5-12-4, Fukushima-ku, Osaka 553, Japan.
Summary:
The population pharmacokinetic profile of vancomycin (VCM) in Japanese pediatric patients infected with methicillin-resistant Staphylococcus aureus was analyzed using 181 samples of serum concentration data from 49 patients obtained in routine drug monitoring. The one-compartment linear model was adopted, where the VCM clearance (CL) and the distribution volume (V d) were correlated with covariates such as postnatal age (AGE) and body weight (BWT). The population pharmacokinetic analysis program NONMEM with the first-order conditional estimation method was used. The results showed that the population mean clearance normalized by BWT increases with AGE up to 1 year of age [CL(L/hour per kg) = 0.119 + 0.0619 · (AGE - 1)] and decreases with age over 1 year old [CL(L/hour per kg) = 0.119 + 0.00508 · (1 - AGE)]. The population mean of the distribution volume normalized by BWT was independent of AGE (V d (L/kg) = 0.522). The interindividual variability of CL was 39.6%, and that of V d was 18.8%. The intraindividual, residual variability was 34.6%. These results were compared with those in other articles, and a guideline for dosage adjustment in VCM therapy is discussed.
Vancomycin (VCM) is a glycopeptide antibiotic generally used for the treatment of gram-positive infections, especially against those caused by methicillin-resistant Staphylococcus aureus(1). The clinical pharmacokinetics of the drug in pediatric patients has been reviewed previously (2) and dosage regimens were discussed for the optimization of VCM therapy. Although side effects of the drug such as nephrotoxicity have been reported in adult patients (3-7), the concentration dependencies of these side effects have not been clarified for pediatric patients (2). In these populations, the VCM dosage should be carefully adjusted because of rapid maturational changes such as developmental changes in total body water volume and kidney function. Therefore, drug concentration monitoring during VCM therapy and the precise evaluation of VCM kinetics should offer useful information for optimizing VCM therapy.
In the pharmacokinetic analysis of VCM in pediatric patients, one- and two-compartment models have often been adopted to describe the serum VCM concentration versus time profile (8-16). Vancomycin is widely distributed in body tissues and fluids and is mainly eliminated unchanged by the kidney via glomerular filtration (2,17,18). Thus change in renal function is one of the important factors affecting VCM kinetics. The glomerular filtration rate is significantly lower in young infants than in children or in adults and gradually increases with age (19-21). Therefore, age is an important covariate affecting the VCM pharmacokinetics.
Recently, we conducted a population pharmacokinetic study of VCM in the course of a postmarketing surveillance study using routine monitoring data and reported the results in adult patients (22). The current article describes the results of the pharmacokinetic analysis of VCM in pediatric patients. Because the serum samples were obtained during the routine drug monitoring and sparse data were available for each patient, we applied the population pharmacokinetic approach to evaluate VCM kinetics in pediatric patient populations. The purpose of the study was to clarify the population pharmacokinetic characteristics of VCM in hospitalized pediatric patients infected with methicillin-resistant S. aureus.
METHODS
Patients and Data Collection
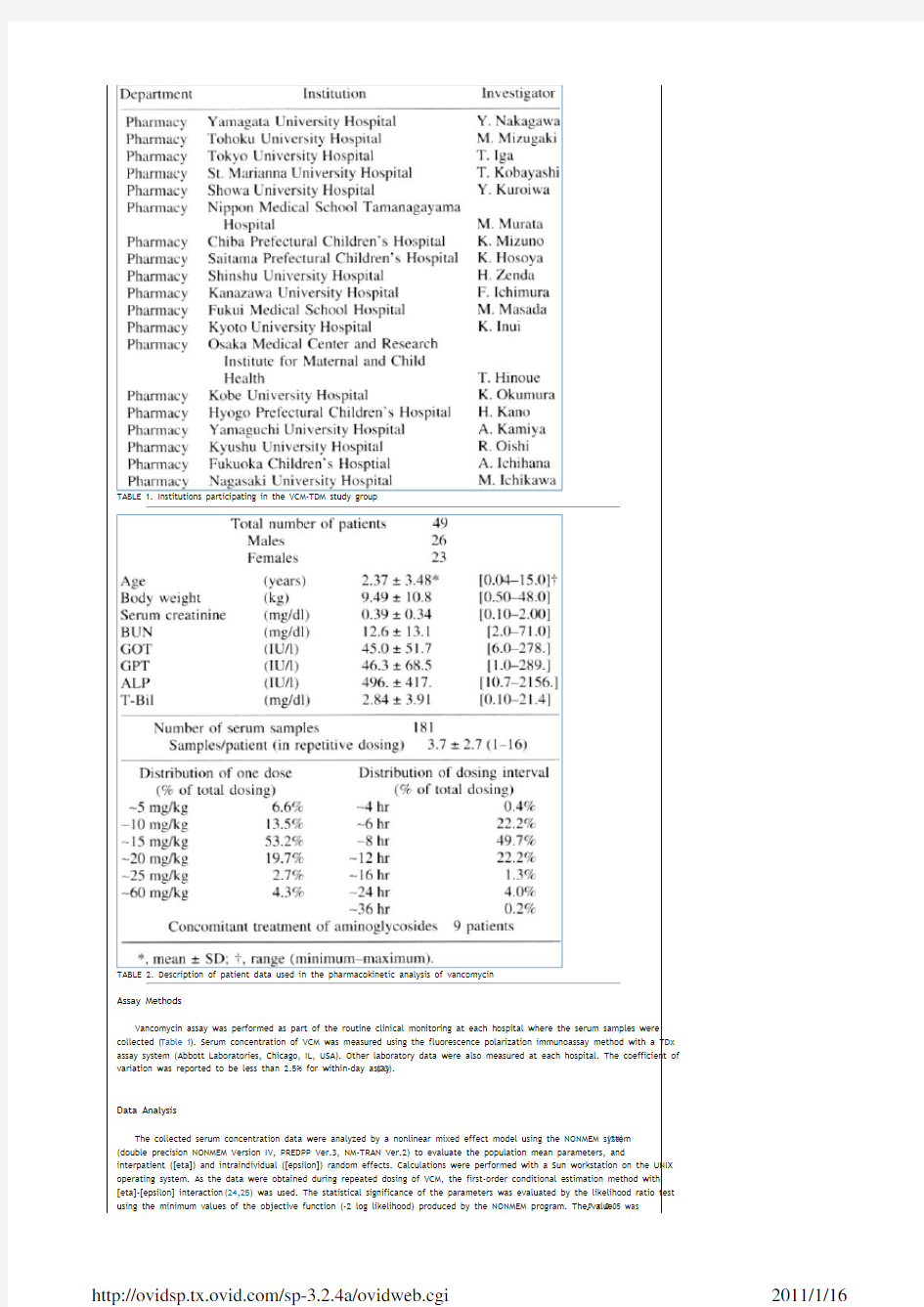
The study was performed with serum concentration data from hospitalized pediatric patients infected with methicillin-resistant S. aureus. The data were collected from patients at the 19 institutions participating in the study group of VCM therapeutic drug monitoring (Table 1) from August 1993 through March 1995. The covariate data collected were gender, postnatal age (AGE), body weight (BWT), and laboratory data including serum creatinine (Scr), blood urea nitrogen, glutamic oxalacetic transaminase, glutamic pyruvic transaminase, alkaline-phosphatase, and total bilirubin. These data were collected at the beginning, end, and appropriate times during VCM treatment. Accurate dosing and serum sampling histories were collected including the dosing date and time, dosing amount, and infusion period from the start of VCM therapy. The demographic data are summarized in Table 2.
TABLE 1. Institutions participating in the VCM-TDM study group
TABLE 2. Description of patient data used in the pharmacokinetic analysis of vancomycin
Assay Methods
Vancomycin assay was performed as part of the routine clinical monitoring at each hospital where the serum samples were collected (Table 1). Serum concentration of VCM was measured using the fluorescence polarization immunoassay method with a TDx assay system (Abbott Laboratories, Chicago, IL, USA). Other laboratory data were also measured at each hospital. The coefficient of variation was reported to be less than 2.5% for within-day assay (23).
Data Analysis
The collected serum concentration data were analyzed by a nonlinear mixed effect model using the NONMEM system (24) (double precision NONMEM Version IV, PREDPP Ver.3, NM-TRAN Ver.2) to evaluate the population mean parameters, and interpatient ([eta]) and intraindividual ([epsilon]) random effects. Calculations were performed with a Sun workstation on the UNIX operating system. As the data were obtained during repeated dosing of VCM, the first-order conditional estimation method with [eta]-[epsilon] interaction (24,25) was used. The statistical significance of the parameters was evaluated by the likelihood ratio test using the minimum values of the objective function (-2 log likelihood) produced by the NONMEM program. The value p < 0.05 was
considered to be statistically significant. Confidence intervals of the estimated population parameters were also calculated using the standard errors obtained by NONMEM.
Pharmacostatistical Model
To determine the basic compartment model, we first fitted both the one- and the two-compartment models with no covariates, and the results suggested the two-compartment model better describes the current data set (difference of the objective functions was 22.5). However, the estimated mean half-life of the [beta]-phase by the two-compartment model was considerably large (about 11 hours), and the numbers of data points throughout the repeated dosing per patient was too small (Table 2) to accurately estimate the two-compartment model parameters. Therefore, we decided to use the one-compartment model using NONMEM PREDPP subroutines ADVAN1 and TRANS1. Vancomycin clearance (CL) and the distribution volume (V d) were used as the basic parameters. The exponential error model for the interindividual variation ([eta]j) was set to the CL and the V d as Equation 1, Equation 2 where TVCL, TVV d are the typical values of CL and V d, respectively, predicted under the regression model with [eta]j equal to zero. The term [eta]j is the random variable for the j th parameter with mean of zero and variances of [omega] 2.
j
Equation 1
Equation 2
For the intraindividual (or residual) variability, the exponential error model was also assumed as follows: Equation 3 where Y and F are the observed and predicted serum concentrations, and [epsilon] is a random variable with mean zero and variance of [sigma]2. The nondiagonal elements of the variance-covariance matrix were ignored.
Equation 3
Development of the Regression Model
The NONMEM system can be used to evaluate the patient [eta]j by the posterior conditional estimation technique (posthoc) using the estimated population mean parameters and the individual observation data, and the individual pharmacokinetic parameter estimates (posthoc estimates) can be obtained in a single NONMEM run. The serum concentration data were first fitted to the one-compartment model with no covariates (i.e. the primitive model), and the mean values and individual posthoc estimates of VCM clearance and V d were simultaneously obtained. Correlation of the covariates such as BWT, AGE, Scr, glutamic oxalacetic transaminase, glutamic pyruvic transaminase, alkaline-phosphatase, and total bilirubin with posthoc VCM clearance and V d were examined by linear regression analysis. The results suggested that VCM clearance significantly (p < 0.05) depends on BWT, AGE, and Scr, and V d significantly depends on BWT and AGE. No significant correlation was found between these VCM pharmacokinetic parameters and the other laboratory data. Pediatric patients are usually classified into three subpopulations according to their postnatal age: newborn (0 to 1 month), infants (1 month to 1 year), and children (older than 1 year of age). As the population in the current study included only one newborn patient, we classified the patients into two groups, i.e. one group including the neonate and infants and the other of children. The volume of total body water normalized by BWT was reported to decrease with age to 1 year and is almost constant in children (19,26,27). Because VCM is a water-soluble compound, this change in total body water may affect the VCM distribution volume. From these preliminary considerations, we assumed the following full model for VCM kinetics in the pediatric patient population.
For neonates and infants: Equation 4, Equation 5
Equation 4
Equation 5
For children: Equation 6, Equation 7
Equation 6
Equation 7
The variables SIZE CL and SIZE Vd are the hypothetical body sizes that represent the nonlinear dependencies of CL and V ss on BWT, and are described as follows: Equation 8, Equation 9
Equation 8
Equation 9
The value of 10 kg was arbitrarily selected for the typical body weight. PF is the factor for correcting the distribution volume normalized by BWT for premature infants, taking the value of 1 for premature infants and 0 for the others. The forward estimation process for the full model was performed in the NONMEM run with the first-order conditional estimation method.
RESULTS
Table 2 summarizes the characteristics of the patients participating in the current study. The data consisted of 181 serum concentration measurements during repeated dosing for 49 patients. There were eight premature infants whose mean body weight and mean postnatal age were 1.01 kg (SD = 0.45) and 0.21 (SD = 0.13) years of age, respectively. The typical dosage was 1 hour infusion of 15 mg/kg and the typical dosage interval for a patient was 8 hours. Nine patients received concurrent treatments with aminoglycosides. However, these drugs were used irregularly and concurrent treatments of these drugs were not included as covariates in the NONMEM analysis. Figure 1 shows the distribution of BWT, AGE, and serum creatinine concentration. The population includes only one neonate, 25 infants, and 23 children. The postnatal age and BWT were closely correlated (r = 0.964). Serum concentration data are shown in Figure 2.
FIG. 1. Distribution of body weight, postnatal age, and serum creatinine of patients studied. [light shade circle] [light shade circle] [light shade circle] : premature infants.
FIG. 2. Serum concentration profile of vancomycin after intravenous infusion. The x-axis is the time from when the infusion was stopped, and all data in each dosing during repetitive administration in all patients were plotted on this scale.
Model building processes are summarized in Table 3. Although the premature factor ([theta]10) was estimated to be significant in the forward estimation processes ([theta]10 = 1.39 (SE = 0.242)), the confidence interval of this parameter included one in the selected model (model 9). The additional calculation (model 13) deleting the parameter from the selected model resulted in no significant increase of the objective function. Therefore, we selected model 13 for the final model. The final estimates of the population pharmacokinetic parameters of VCM are shown in Table 4. The estimated VCM clearance by posthoc estimation using the final model is shown in Figure 3. The size factors for both CL and V d ([theta]8 and [theta]9) were not significantly different from 1, i.e., CL and V d were linearly correlated with BWT, and V d was independent of AGE when normalized by BWT. In contrast, VCM clearance normalized by BWT depended on AGE, and increased with AGE in infants, and decreased with AGE in children. These results coincide with the age-related maturational process of kidney function in younger pediatric patients (up to 1 year) (19-21).
TABLE 3. List of models tested and log likelihood differences
TABLE 4. Final population pharmacokinetic parameter estimates of vancomycin in pediatric patients
FIG. 3. Estimated vancomycin clearance in each patient by posthoc estimation using the final model. The line represents the population mean value.
Figure 4 shows the relationship between the observed concentration and the predicted values by the posthoc estimation using the final model. Comparably good correlation was found for the concentration range below 40 μg/ml, but some points were overestimated at a higher concentration range. This is because the one-compartment model was adopted here and the distribution phase of VCM soon after infusion was terminated could not be clearly explained by the one-compartment model.
FIG. 4. Relationship between the observed vancomycin concentration and estimated values by the posthoc prediction using the final model. The line of identity is shown.
DISCUSSION
In this work, we estimated the population pharmacokinetic parameters of VCM using sparse serum concentration data obtained from routine monitoring. There have been some reports concerning pharmacokinetic evaluation of VCM in pediatrics, and the estimated parameters were recently reviewed (2). The parameters estimated in the current study generally agreed with these previously reported values. For example, Schaad et al (8) reported the [beta]-phase half-life (t?([beta])) to be 4.1 hours for infants and 2.2 to 3.0 hours for children 3 to 7 years old. The calculated mean half-life of infants in the current study was 6.3 hours (0 year) and 3.0 hours (1 year) and 2.8 hours for children of 3 years of age.
Although Scr was found to be a significant factor affecting VCM clearance by the linear regression analysis, the final model does not include Scr as a covariate. One of the reasons for this result is the small number of patients with high Scr levels included in the analysis. Some articles reported the correlation of VCM clearance of infants with indexes of kidney function such as serum creatinine level (11) and creatinine clearance (15).
According to the final parameter estimates, we simulated an example of the optimum dosage regimen. When the target peak (strictly speaking, the serum concentration at 1 hour after the infusion was terminated) and trough concentrations were set, the optimum infusion rate (Rate*) and dosing interval ([tau]*) were calculated using the following equations: Equation 10, Equation 11 where C peak and C trough are the target peak and trough concentrations, Ke is the elimination rate constant ( = CL/V d) and T inf is the infusion period. Figure 5 shows an example in which the target peak and trough concentrations were set at 35 and 10 μg/ml, respectively. In most patients, the desired infusion rate is about 15 mg/kg per hour. The recommended dosing intervals were from 8 to 16 hours, and the 8-hour interval seems to be preferable for patients approximately 1 year of age.
Equation 10
Equation 11
FIG. 5. An example of the optimum dosage interval (upper) and the optimum infusion rate (lower) in pediatric patients. The target peak and trough were set at 35 and 10 μg/ml, respectively. An infusion period of 1 hour was assumed. The curves are the optimum values calculated using the population mean parameters and each plot represents the optimum interval and infusion rate based on the posthoc parameter estimates of each patient.
Much attention has been paid to the pharmacokinetics and dosage regimens in low-birth weight neonates or infants (9,10,28-30). The current results did not include enough information about this population. Speculating from the results in Figure 5 at the age of 0, the recommended dosing interval is about 12 hours and infusion rate is from 15 to 20 mg/hour per kg. Although the correction factor for premature infants ([theta]10) could not be precisely obtained from the current analysis, some corrections for V d might be required for premature infants because of their low body weight compared with the normal value.
In summary, we studied the population pharmacokinetics of VCM using serum concentration data obtained in routine monitoring during post marketing surveillance. As Bayesian forecasting offers many important advantages for dosage individualization (31), the current results should be useful for estimating the initial dosage and for Bayesian forecasting in routine drug monitoring and VCM therapy.
APPENDIX
At steady state, the peak concentration (1 hour after infusion terminated, C peak) and the trough concentration (C trough) are given by equations (A1) and (A2).
Equation A1
Equation A2
From equation (A1), the optimum infusion rate (Rate*) is obtained as shown by equation (10). By dividing C peak (equation A1) with C trough (equation A2), the optimum dosing interval ([tau]*) can be given as equation (11).
REFERENCES
1. Sorrell TC, Packham DR, Shanker S, Foldes M, Munro R. Vancomycin therapy for methicillin-resistant. Staphylococcus aureus. Ann Intern Med 1982;97:344-50. Full Text Bibliographic Links Library Holdings[Context Link]
2. Rodvold KA, Everett JA, Pryka RD, Kraus DM. Pharmacokinetics and administration regimens of vancomycin in neonates, infants, and children Clin Pharmacokinet 1997;33:32-51. [Context Link]
3. Traber PG, Levine DP. Vancomycin ototoxicity in a patient with normal renal function. Ann Intern Med 1981;95:458-60. Full Text Bibliographic Links Library Holdings[Context Link]
4. Levine DP, Cushing RD, Jui J, Brown WJ. Community-acquired methicillin-resistant staphylococcus aureus endocarditis in the Detroit Medical Center. Ann Intern Med 1982;97:330-338. Full Text Bibliographic Links Library Holdings[Context Link]
5. Ryback MJ, Albercht LM, Boike SC, Chandrasekar PH. Nephrotoxicity of vancomycin, alone and with an aminoglycoside. J Antimicrob Agents Chemother 1990;25:679-87. [Context Link]
6. Cimino MA, Rotstein C, Slaughter RL, Emrich LJ. Relationship of serum antibiotic concentrations to nephrotoxicity in cancer patients receiving concurrent aminoglycoside and vancomycin therapy. Am J Med 1987;83:1091-
7. Full Text Bibliographic Links Library Holdings[Context Link]
7. Bryan KV, Rotschafer JC, Gilliland SS, Rodvold KA, Fitzgerald CM, Guay RP. A comparative assessment of vancomycinized patients. J Antimicrob Chemother 1994;33:811-821. Library Holdings[Context Link]
8. Schaad UB, McCracken GH, Nelson JD. Clinical pharmacology and efficacy of vancomycin in pediatric patients. J Pediatr
1980;96:119-26. Full Text Bibliographic Links Library Holdings[Context Link]
9. James A, Koren G, Milliken J, Soldon S, Prober C. Vancomycin pharmacokinetics and dose recommendations for preterm infants. Antimicrob Agents Chemoter 1987;31:52-4. [Context Link]
10. Lisby-Sutch SM, Nahata MC. Dosage guidelines for the use of vancomycin based on its pharmacokinetics in infants. Eur J Clin Pharmacol 1988;35:637-642. Full Text Bibliographic Links Library Holdings[Context Link]
11. Kildoo CW, Lin LM, Gabriel MH, Folli HL, Modanlou HD. Vancomycin pharmacokinetics in infants: relationship to postconceptional age and serum creatinine. Dev Pharmacol Ther 1990; 14:77-83. [Context Link]
12. Asbury WH, Darsey EH, Rose WB, Murphy JE, Buffington DE, Capers CC. Vancomycin pharmacokinetics in neonates and infants: a retrospective evaluation. Ann Pharmacother 1993;27:490-6. Bibliographic Links Library Holdings[Context Link]
13. Chang D, Liem L, Malogolowkin M. A prospective study of vancomycin pharmacokinetics and dosage requirement in pediatric cancer patients. Pediatr Infect Dis J 1994;13:969-74. Ovid Full Text Request Permissions Full Text Bibliographic Links Library Holdings[Context Link]
14. Seay RE, Brundage RC, Jensen PD, Schilling CG, Edgren BE. Population pharmacokinetics of vancomycin in neonates. Clin Pharmacol Ther 1994;56:169-75. Full Text Bibliographic Links Library Holdings[Context Link]
15. Rodvold KA, Gentry CA, Plank GS, Kraus DM, Nickel E, Gross JR. Bayesian forecasting of serum vancomycin concentrations in neonates and infants. Ther Drug Monit 1995;17:239-46. Ovid Full Text Full Text Bibliographic Links Library Holdings [Context Link]
16. Chang D. Influence of malignancy on the pharmacokinetics of vancomycin in infants and children. Pediatr Infect Dis J
1995;14:667-73. Ovid Full Text Request Permissions Full Text Bibliographic Links Library Holdings[Context Link]
17. Leader WG, Chandler MHH, Castiglia M. Pharmacokinetics optimization of vancomycin therapy. Clin Pharmacol 1995;28:327-42. Library Holdings[Context Link]
18. Matzke GR, Zhanel GG, Guay DRP. Clinical pharmacokinetics of vancomycin. Clin Pharmacokinet 1986;11:257-82. Full Text Bibliographic Links Library Holdings[Context Link]
19. Evans WE, Schentag JJ, Jusko WJ, Harrison H, eds. Applied pharmacokinetics, ed 2. Spokane, WA: Applied Therapeutics, 1986:249-330. [Context Link]
20. Barnett HL. Kidney function in young infants. Pediatrics 1950;5:171-9. Bibliographic Links Library Holdings[Context Link]
21. Hook JB, Bailie MD. Perinatal renal pharmacology. Ann Rev Pharmacol Toxicol 1979;19:491-509. Full Text Bibliographic Links Library Holdings[Context Link]
22. Yasuhara M, Iga T, Zenda H, et al. Population pharmacokinetics of vancomycin in Japanese adult patients. Ther Drug Monit 1998;20:139-48. [Context Link]
23. Prescribed Information of TDx-Vancomycin. Chicago: Abbott Laboratories, U.S.A. [Context Link]
24. Beal SL, Sheiner LB, eds. NONMEM users' guides. NONMEM Project Group, University of California at San Francisco, 1992. [Context Link]
25. Mandema KM. Population pharmacokinetics and pharmacodynamics. In: Welling PG, Tse FLS, eds. Pharmacokinetics. New York: Mercel Dekker, 1995:411-50. [Context Link]
26. F-Hansen B. Body water compartments in children. Changes during growth and related changes in body composition. Pediatrics 1961;28:169-81. Bibliographic Links Library Holdings[Context Link]
27. F-Hansen B. Body composition during growth. In vivo measurements and biochemical data correlated to differential anatomical growth. Pediatrics 1971;47:264-74. Full Text Bibliographic Links Library Holdings[Context Link]
28. Schable DH, Rocci ML, Alpert GA, et al. Vancomycin pharmacokinetics in infants: relationship to indices of maturation. Pediatr Infect Dis 1986;5:304-308. Library Holdings[Context Link]
29. Leonard MB, Koren G, Stevenson DK, Prober CG. Vancomycin pharmacokinetics in very low birth weight neonates. Pediatr Infect Dis 1989;8:282-6. Ovid Full Text Library Holdings[Context Link]
30. Gabriel MH, Kildoo CW, Gennrich JL, Modablou HD, Collins SR. Prospective evaluation of vancomycin dosage guidelines for neonates. Clin Pharm 1991;10:129-32. Bibliographic Links Library Holdings[Context Link]
31. Gatta MF, Garcia MJ, Lanao JM, D-Gil A. Bayesian forecasting in pediatric populations. Clin Pharmacokinet 1996;31:325-30. [Context Link]
Key Words: Population pharmacokinetics; Vancomycin; Pediatric patients; Methicillin-resistant Staphylococcus aureus (MRSA); NONMEM; Dosage guideline
IMAGE GALLERY
Select All
Export Selected to PowerPoint
Table 1
Table 2
Equation 1
Equation 2
Equation 3
Equation 4
Equation 5
Equation 6
Equation 7
Equation 8
Equation 9
Fig. 1
Fig. 2
Table 3
Table 4
Fig. 3
Fig. 4
Equation 10
Equation 11
Fig. 5
Equation A1
Back to Top
Copyright (c) 2000-2010 Ovid Technologies, Inc.
Terms of Use Support & Training About Us Contact Us
Version: OvidSP_UI03.02.04.102, SourceID 52749
考点: 1. 掌握可数名词的复数 2. 学会表示不可数名词的量 3. 掌握构词法:名词变形容词 4. 掌握名词所有格的用法 5. 掌握名词做主语、定语的用法 冠词离开名词没有任何意义,因此在学习冠词前,首先要了解名词的分类: '个体名词:人或物所共用的名称 dog, chair 名词可分为::可数名词v 丄集体名词:集体的名称 class, family, police, 物质名词:物质的名称 p aper, water 抽象名词:抽象的物的名称 happi ness 专有名词:人或物所特有的名称 Tom, China 考点一:可数名词的数 可数名词复数变化规则: (1) 规则变化:a.以-s,-x,-sh, -ch,结尾的名词,在词尾 +es,发音/-Is/ eg : classes, brushes, boxes, watches b. 以辅音字母+ -y 结尾,将y 变i ,再+es , eg : parties, stories (注意元音同y 结尾时+s boys ) c. 部分以f 或fe 结尾的词,将变 f/fe 为v+es , eg : wife-wives 口诀:(妻见小偷加下藏,手拿小刀想杀狼,忽然飘下一片叶,砸在头上一命亡) d. 部分以o 结尾的词,(生物名词,包括动植物,口诀:黑人英雄爱吃土豆西红柿)后加 es , 女口: Negroes, heroes, potatoes, tomatoes, 以o 结尾的无生命的词,一般直接 +s eg : photos , pianos , kilos , tobaccos (2) 不规则变化: a.名词中所含元音字母发生变化 eg: foot-feet; tooth- teeth; man-men; woma n- wome n; b:名词词尾力口 en/ren : ox-oxen ; child-children ; c. 单复数同行: fish; sheep; deer; means; aircraft; d. 关于国家:中日不变,英法荷变,其他后面加 s two Chin ese; five Japa nese;/ En glishme n; En glishwome n; Dutchme n; /Germa ns; America ns e. 有些集体名词用单数形式表达事物总称 ,如hair, fruit,但在 表示"几根头发”,"若 干水果”时,则用复数形式 a few white hairs; several foreig n fruits f. 有些名词形式上是单数的,但实际上是复数的,这一类名词有:cattle 牛, 家畜;people 人 们;vermin 害虫;police 警察;staff 全体职员;clergy 僧侣,神职人员;youth ; mankind ; bacteria ; crew 等 g. 有些集体名词 表示整体时用单数,表示集体中的各个成员时用做复数 ,能这样用的 集体名词有: audienee , club , class, college , crowd , company , couple , department , enemy , family , firm , flock, generation, government, group, herd, navy, party, public, population, press 新闻界 /记者群, staff, team, university 等 (3) 复合名词的复数 a.由man 或woman 为前缀的复合名词,两者都变成复数 a man teacher/ men teachers ; a woman doctor/ women doctors 名词 I 不可数名词
不定代词讲解~详细 一、不定代词some 与any 的用法区别 一般说来,不定代词some 用于肯定句中,any 用于否定句和疑问句中。但是,在表示请求、邀请或征求意见的句子中,通常要用some 而不用any: Would you like some cake? 吃点蛋糕吗? Why not buy some bread? 为什么不买些面包呢? Shall I get some chalk for you? 要我帮你拿些粉笔来吗? 【说明】不定代词any 有时也用于肯定句中,此时表示“任何”: Any colour will do. 任何颜色都行。Come any day you like. 随便哪天来都可以。 二、不定代词many 与much 的用法以及区别 不定代词many 和much 都表示“许多”,但many 修饰或代替可数名词(复数),与few(少数)相对;而much 用来修饰或代替不可数名词(单数),与little(少量)相对。在口语中两者主要用于非肯定句中: Did you see many people there? 你在那儿看见许多人了吗? We don’t have much time. 我们没有许多时间。 Much work has been done. 许多工作都已经做了。 You’ve given me too much. 你已给我太多了。 Take as many (much) as you want. 你要多少拿多少。 I asked her a great many questions. 我问了她许多问题。 辨析:too much;much too;too many 1、too much常用作副词或代词,也可以用作形容词修饰不可数名词.如: Is watching TV too much good or bad for your health?电视看得太多对你的健康有益还是有害? You've given me too much.你给我的太多了. We've had too much rain lately.最近我们这里的雨下得太多了. 2、much too常作副词,后接副词或形容词.如: He drove much too fast.他开车开得太快了. It is much too cold.天实在太冷了. 3、too many常用作形容词,修饰可数名词复数.如: They built too many buildings last year.去年他们建了许多楼房. 三、either、neither的用法以及区别 1、用作副词。either也(不),用于否定句中。 如:I don’t like fishing, David doesn’t like fishing, either.我不喜欢钓鱼,大卫也不喜欢。 neither也不;用于肯定句,表示否定含义。如:He can’t swim, and neither / nor can I. 他不会游泳,我也不会。 2、用作代词。范围多限定于两者之间,常用作主语。either of 和neither of +名词/代词的复数,作主语时,谓语动词用单数。 either表示“二者之一”;neither 表示“两者都不”,其反义词是both。 如:Either of the knives is useful.两把刀都有用。 Neither of them was in good health, but both worked very hard.他们两人身体都不好,但都努力地工作。 3、用作连词:either…or…不是……就是……neither…nor…既不……也不……常用来连接两个并列成分,如并列主语、并列谓语等。谓语动词保持就近原则,与离它最近的主语在人称和数上保持一致。 但应注意以下几点: 1.无论either…or…还是neither…nor…,若连接两个单数数名词/代词作主语,后面动词用单数。 Either Mary or Lucy is coming.不是玛丽来,就是露西来。 2.若连接两个复数名词/代词作主语,后面动词用复数。Neither my parents nor my grandparents are coming. 我的父母不来,我的爷爷奶奶也不来。 3.如果一个单数名词/代词和一个复数名词/代词一起作主语时,动词的单复数形式必须和最靠近的一个主语保持一致。(就近原则)
最新英语非谓语动词用法总结(完整) 一、单项选择非谓语动词 1.Students surf the internet _______ more information about the university they are dreamt of. A.found B.finding C.having found D.to find 【答案】D 【解析】考查非谓语动词。句意:学生们上网是为了找到他们理想大学的更多的信息。此处表示目的用不定式,指上网的目的。故选D。 2.Look over there! There is a long, winding path ________ up to the house. A.lead B.leading C.led D.to lead 【答案】B 【解析】 【详解】 考查非谓语动词。句意:看那边!有一条长长的蜿蜒小路通向那所房子。分析句式可知,这是个there be 句型,因此,此处用非谓语动词,path与lead是主动关系,因此用现在分词,故选B。 3.______ to nuclear radiation, even for a short time, may influence genes in human bodies. A.Having exposed B.Being exposed C.To expose D.Exposed 【答案】B 【解析】 【详解】 考查动名词。句意:暴露于核辐射中甚至很短时间都会影响人体的基因。分析句子成分发现even for a short time是插入语,may influence是谓语,前面的部分应该是主语,be exposed to“暴露于”,要用动名词Being exposed to。故B选项正确。 4.The lecture, _______at 7:00 pm last night, was followed by an observation of the moon with telescopes. A.starting B.being started C.to start D.to be started 【答案】A 【解析】 选A start与逻辑主语the lecture之间为主动关系,故排除B、D两项。不定式作定语时,常表示动作尚未发生,故排除C项,此处用现在分词作后置定语,表示主动。 第四步:根据与谓语动词的先后关系确定时态 非谓语动词表示的动作发生在谓语动词表示的动作之前用过去分词或v.-ing形式/不定式的
Population population是一个集合名词,它的用法有时较为特殊,很容易用错。 一、population常与定冠词the连用,作主语用时,谓语动词常用第三人称单数形式。例如: The world's population is increasing faster and faster. 全世界的人口增长得越来越快。 At the beginning of the twentieth century, the world's population was about 1,700 million. 在二十世纪初,全世界的人口大约是十七亿。 二、当主语是表示"人口的百分之几、几分之几"时,谓语动词用复数形式。例如: About seventy percent of the population in China are farmers. 中国大约有百分之七十的人口是农民。 三、有时population可用作可数名词,其前可用不定冠词。例如: China has a population of about 1.3 billion. (=There is a population of about 1.3 billion in China.) 中国大约有十三亿人口。
New York is a big city with a population of over 10 million. 纽约是一个有一千多万人口的大城市。 补:在表示多个地区的人口时,population要用复数形式populations。例如: Many parts of the world, which once had large populations and produced plenty of crops, have become deserts. 世界上很多地区一度人口众多,种植大量的农作物;现在,这些地区已经变成了沙漠。 四、表示人口的"多"或"少",不用"much"或"little",而要用"large" "big"或"small"。例如: India has a large population. 印度人口众多。 Singapore has a small population. 新加坡人口少。 五、询问某国、某地有多少人口时,不用"How much...?",而用"How large...?";在问具体人口时用"What...?"。例如: -How large is the population of your hometown? 你们家乡有多少人口?
不定代词总结 一、不定代词 some 与 any 的用法区别 一般说来,不定代词 some 用于肯定句中, any 用于否定句和疑问句中。但是,在表示请求、邀请或征求意见的句子中,通常要用 some 而不用 any : Would you like some cake? 吃点蛋糕吗? Why not buy some bread? 为什么不买些面包呢? Shall I get some chalk for you? 要我帮你拿些粉笔来吗? 【说明】不定代词 any 有时也用于肯定句中,此时表示“任何”: Any colour will do. 任何颜色都行。 Come any day you like. 随便哪天来都可以。 二、不定代词 many 与 much 的用法以及区别 不定代词 many 和 much 都表示“许多”,但 many 修饰或代替可数名词(复数),与 few(少数)相对;而 much 用来修饰或代替不可数名词(单数),与 little(少量)相对。在口语中两者主要用于非肯定句中: Did you see many people there? 你在那儿看见许多人了吗 ? We don 't have much time. 我们没有许多时间。 Much work has been done. 许多工作都已经做了。 You 've given me too much. 你已给我太多了。 Take as many (much) as you want. 你要多少拿多少。 I asked her a great many questions. 我问了她许多问题。 辨析: too much ; much too ; too many 1、too much 常用作副词或代词 ,也可以用作形容词修饰不可数名词 .如: Is watching TV too much good or bad for your health? 电视看得太多对你的健康有益还是有害 ? You've given me too much. 你给我的太多了 .
高考英语非谓语动词用法总结(完整) 一、单项选择非谓语动词 1.The rainforest is an amazing place, ________ with plants and animals that aren’t found anywhere else in the world. A.filling B.filled C.being filled D.to fill 【答案】B 【解析】考查非谓语动词。句意:热带雨林是一个令人惊讶的地方,充满了世界其他地方不能找到的动植物。固定词组:be filled with被……充满,此处place和fill之间是一种被动关系,所以用过去分词做伴随状态,故选B。 2.115.______ his love, Chris sent his mom a thank-you note on Mother’s Day. A.Expressing B.Expressed C.To express D.Having expressed 【答案】C 【解析】考查动词不定式。句意:为了表达他的爱,克里斯在母亲节那天给他的妈妈寄了一条感谢信。用不定式表目的,故选C。 3.After receiving the Oscar for Best Supporting Actress, Anne Benedict went on all the people who had helped in her career. A.to thank B.thanking C.having thanked D.to have thanked 【答案】A 【解析】 试题分析:句意:在获得奥斯卡最佳女配角后,Anne Benedict继续感谢所有帮助她演绎生涯的人。go on to do继续做不同的事情,所以选A。 考点:考查不定式 【名师点睛】不定式有一些具体的用法,可以做宾语,定语,状语。还有不定式的不同形式:to do;to be doing;to have done。这题要注意go on to do“继续做不同的事情”和go on doing“继续做相同的事情”的区别。结合语境是关键。 4.Pressed from his parents, and ____ that he has wasted too much time, the boy is determined to stop playing video games. A.realizing B.realized C.to realize D.being realized 【答案】A 【解析】 试题分析:考查非谓语动词的用法。句意:被父母迫使同时自己也意识到他已经浪费了太多时间,这个男孩决定停止玩电脑游戏。首先要弄清楚本句中的and连接的成分是非谓语
不定代词用法总结-标准化文件发布号:(9556-EUATWK-MWUB-WUNN-INNUL-DDQTY-KII
不定代词用法总结 1) some, any, no的用法 a. some和any通常用于表示不定数或不定量,修饰复数可数名词或不可数名词。some表示“几个;一些;部 分”,多用于肯定句;而any表示“一些;什么;任何;”,对用于否定句或疑问句中。如: * He asked me some questions. (他问了我几个问题。) * Some of the bread has been eaten. (面包已吃了一些。) * Are there any stamps in this post office (这个邮局里有邮票吗?) * I didn’t have any cigarettes, so I went out to buy some. (我没有香烟了,所以出去买了一些。) b. 刚才我们说some一般用于肯定句而any一般用于否定句和疑问句。但有时也有例外。这要根据句子意思来 看。 * I could not answer some of his questions. (我不能回答他的某些问题。) (some用在否定句中表示“一些;部分”。如果说成:I could not answer any of his questions.意思就变了,它表示“我不能回答他的任何问题。”) * Will you get me some apples on your way back (你回来的路上能给我带一些苹果吗?) (some用在疑问句中大多表示“请求” 或“建议”) * Let me know if you hear any news. (如果你有任何消息请告诉我。) (any用在条件从句中表示“任何”) * “What would you like to drink” “Any will do.” (“你想喝什么?”“哪种都行。”) (any在这里表示“任何”) c. no在句子中作定语,表示否定,意思是“没有;不是”,它可以修饰可数名词的单数和复数形式或不可数名 词。 * There are no letters for you today. (今天没有你的信。) * I have no money at the moment. Could you lend me some (我现在没有钱。你能借我一些吗?) 2) 复合不定代词的用法 a. 不定代词some, any, no与-one, -body, -thing可以组成九个复合代词。它们是: someone anyone no one somebody anybody nobody something anything nothing 这些复合不定代词只有名词的性质,可以作主语、宾语等。 b. 因为some一般用于肯定句,any一般用于否定句或疑问句,no表示完全否定,因此由some, any, no与-one, - body组成的复合代词的用法也一样。 c. 第二部分为-one和-body的复合代词只用于表示人,它们的形式是单数形式,但有时可以用they或them指 代。 * There is someone in your office. Can you hear them talking (你办公室里有人。你听见他们说话了吗?) d. 第二部分为-thing的复合代词只能用于指物。如: * There was something wrong with the car so he had to stopped it. * He looked at me and didn’t say anything. * Nothing can be done to save her life. e. 这些复合不定代词如果有其它的形容词修饰,形容词必须后置。如: * Somebody important has arrived, I’m sure. (important修饰somebody) 3) one和none的用法 不定代词one指代可数名词的单数,即指人,也指物。它的复数形式是ones。在句中可以作主语、宾语、定语等。 * He is not the one who is easily cheated. (one指人) * I’ve made some cakes. Would you like one of them (one指物) * I prefer red roses to white ones. (ones指物) * Are they the ones who moved here a few days ago (ones指人) 4) all, every, each, other, another, either, neither, both a. every只有形容词的性质,在句中作定语。常用于修饰单数的可数名词。表示“每个;各个”,还可以表示“一 切”。 * After the strong wind every flower in the garden was gone. every还可以和-one, -thing, -body构成复合不定代词,即:everyone, everything, everybody。其中,everyone和everybody用于指人,意思一样,都是“每人;大家”,形式上表示单数意思上可以表示单数也可以表示复数。everything用于指物,意思是“每件事;一切”,形式上表示单数意思上可以表示单数也可以表示复数。如:* One can’t have everything. * Everything goes well with me. * The town is so small that everybody knows everybody else. 注意:在使用everyone时要注意和every one相区别。everyone是一个不定代词而every on是一个词组,前者只能指人而后者既可以指人也可以指物。请注意下列例句: * Everyone will be here except Patrick. (everyone 指人) * Every one of the children will get a gift. (every one也指人) *We played several matches against the visitors, but unluckily lost every one. (every one指物)
Module 9 Population 词汇精讲 1. noise ,voice &sound (1)noise 可以作可数名词,也可以用作不可数名词,表示“人们不愿听到的声音或嘈杂声”。 例如: I heard some strange noises last night. 昨夜我听见一些奇怪的响声。 There's a lot of noise here. 这个地方人声嘈杂。 (2)voice 作名词,意为“声音,嗓音”。用于人时,指说话、歌唱或发笑的声音,也可指发言权。用于其它方面时,常含悦耳之声,如鸟鸣声,乐器声音等。例如:He talked of his trip to Hong Kong in a cheerful voice. 他兴高采烈地谈了他的香港之行。 She has a sweet voice. 她声音很甜美。 (3)sou nd泛指自然界的任何声音,不论其高低、是否悦耳等。例如: I heard the sound of running water. 我听见流水声。 Light travels faster than sound. 光比声音传播得快。 2. huge huge 是常用词, 用于具体事物或人时, 指“体积或数量大得超过一般情况” ;用于抽象事物时, 作“巨大的”、“无限的”解。例如: He stood tongue-tied before the huge audience. 在大批听众面前他站着说不出话来。 【拓展】 (1)big “大的,巨大的”,常指程度,范围,规模,容积,重量,数量等(还可表示“伟大,重要”之意)常可与large 互换,多用于具体的、有形的人或物(其反义词多为 little/small 。) 例如:There is a big tree beside the house.房子旁边有一棵大树。 (2)great 大“的,极大的,伟大的,重要的,超乎寻常”,常指面积,数量,程度(或指抽象的东西,如知识,能力,人格等),用来指人时,表示“伟大的,杰出的”,其反义词为little/small 。例如: We heard a great n oise我们听到一个很大的响声。 【注意】big还可以作长大了”解,great有时可表达说话人的喜悦、赞扬等感情。 例如:Lily is big enough to ride a bike. 莉莉长大了,可以骑自行车了。 He's the greatest man I have ever seen. 他是我见过的最伟大的人物。 (3)large “大的,巨大的”,常指面积,范围,可表示数和量(当它直接用于人时,可表示身体的大),其反义词为small。例如: They say China is a large and beautiful country. 他们说中国是一个面积大而美丽的国家。 3. question&problem question 和problem 都有“问题”的意思,但用法不同。question 指须解答的问题,是就疑问而言的;problem 指须解决的问题,是就困难而言的。例如: What's your question? Can you answer it? 你的问题是什么?你能自己回答吗? What's your problem? Can you solve it by yourself? 你的问题(困难)是什么?你能自己解决吗? 4. billion (1)billion是数词,意为十亿”当表示具体的几十亿”时,用基数词+ billion ,注意不加-s。 第 1 页
不定代词用法归纳(详细讲解) ■本站特约作者陈根花 一、不定代词概说 英语的不定代词有 all, each, both, either, neither, one, none, little, few, many, much, other, another, some, any, no, (a) few, (a) little, both, enough, every 等,以及由 some, any, no 和 every 构成的合成代词(即somebody, anyone, nothing 等)。在这些不定代词中,多数都能作主语、宾语、表语或定语,但是代词 none 以及由 some, any, no 和 every 构成的合成代词只能作主语、宾语或表语,不能作定语,而 no 和 every 则只用作定语。 二、指两者和三者的不定代词 有些不定代词用于指两者(如both, either, neither),有的不定代词用于指三者(如all, any, none, every),注意不要弄混: Both of my parents are doctors. 我的父母都是医生。 All of the students are interested in it. 所有的学生对此都很感兴趣。 There are trees on any side of the square. 广场的每一边都种有树。 He has two sons, neither of whom is rich. 他有两个儿子,都不富有。 He has three sons, none of whom is rich. 他有三个儿子,都不富有。 【说明】each 可用于两者、三者或三者以上,而 every 只用于三者或三者以上,因此用于两者时只能用 each,不能用 every。如不能说 There are trees on every side of the road. 三、复合不定代词的用法特点 复合不定代词包括 something, somebody, someone, anything, anybody, anyone, nothing, nobody, no one, everything, everybody, everyone 等。它们在句中可用作主语、宾语或表语,但不能用作定语。something, someone 等和 anything, anyone等的区别与 some 和 any 的区别一样,前者一般用于肯定句,后者一般用于否定句、疑问句或条件句(参见 any & some)。具体使用时应注意以下几点: 1.复合不定代词受定语修饰时,定语应放在它们后面: There is nothing wrong with the radio. 这收音机没有毛病。 Have you seen anyone [anybody] famous? 你见过名人吗? 2.指人的复合不定代词若用作主语,其谓语动词一般用单数,相应的人称代词和物主代词也用单数 he, him, his (不一定指男性)。但在非正式文体中常用复数代词 they, them, their:Everyone knows this, doesn’t he [don’t they]?人人都知道这一点,不是吗? If anybody [anyone] comes, ask him [them] to wait. 要是有人来,让他等着。 3.指事物的复合不定代词若用作主语,谓语动词只能用单数,相应的人称代词也只能用 it,而不用 they:
非谓语动词的用法总结 李靖 非谓语动词(不定式、动名词、分词)不是真正意义上的谓语动词,在句中都不能单独作谓语。但都具有动词的某些特点,可以有自己的宾语或状语,构成非谓语动词短语。不定式表目的,表将来;动名词表主动,表进行;过去分词表被动,表完成。 一.作主语( 动名词、不定式、过去分词前面加being, 动名词做主语谓语动词用单数) 1)不定式、动名词都可做主语,但是动名词做主语多指抽象的概念性的动作,可以是多次的经常的行为;不定式多表示具体的动作,尤其是某一次的动作。如: Playing with fire is dangerous. 玩火危险。(泛指玩火) To play with fire will be dangerous. 玩火会发生危险。 2)用动名词做主语的句型: It’s no use/no good/pleasure doing sth 做.......没有用处/好处/乐趣 It’s a waste of time doing sth 做.... 浪费时间 It is worth doing sth 值得做某事 It is no use crying over spilt milk. 覆水难收 It is worth making an appointment before you go. 去之前预约一下是值得的。 3)不定式做主语的句型. It is + adj +for sb to do sth. 比较:表示人的品质时只能用of sb 如considerate/kind/nice/foolish/stupid/rude/cruel /wise/clever/brave/selfish/crazy/good/careful/careless/impolite/right/wrong等单词出现 时。 It is silly of you to say so. It is important for us to learn English well. It is a must/ a necessity for us to have a good command of the English language. 4) “Wh- + to 不定式”可做主语。如: When to leave hasn’t been decided yet.什么时候动身还没定呢。 Whether to drive or take the train is still a problem.是自驾车还是乘火车仍是一个问题。 5)一般情况下,不定式和动名词作主语,谓语动词一般用单数形式。如: Seeing is believing.= To see is to believe 眼见为实。 . Planting flowers needs constant watering. 但and连接的多个动名词作主语,谓语动词大多用复数(如果前后动名词的语义一致, 谓语一般用单数)。如:Lying and stealing are immoral. 说谎与盗窃是不道德的。 6) 动名词前面可以加上形容词性物主代词构成动名词的复合结构。如: ----- What made him angry? ------ Mary’s /My/His/Her /Their/ The boy’s/ The president’s being late(made him angry. 7being,构成动名词,做主语。如: . Being examined twice a year , driver must obey in this city. 经典练习:
不定代词用法一览表 例词含义作用例句 both 后接复数名词表示 两个 人或 事物 主语Both are teachers. 两个都是教师。 宾语 The teacher wanted both of us to go.老师要我们两个 人都去。 定语Both questions are easy.两个问题都很容易。 同位语They both did it well.他们两个人都干得不错。 注: 1. both与定冠词、指示代词、物主代词连用时,应放在这些词的前面。 2. both在否定句中用作主语时,表示部分否定。如: Both of you won’t go. 你们两个不需要都走。 neithe r 后接单数名词(与both 反义) 表示 两个 人或 事物 都不 主语Neither is mine.两个都不是我的。 宾语I want neither of the books.那两本书我都不要。 定语Neither sentence is correct.两个句子都不对。 注: Neither在句子中作主语时,谓语动词用单数形式。Neither在 句子中作主语时表示全部否定。如: Neither of you is Japanese.你们两个都不是日本人。 You can’t eat either of them=You can eat neither of them. either 后接单数名词两个 人或 物中 任一 个 主语Either will be all right.两个中哪一个都行。 宾语 He looked at the two pens, but didn’t buy either(=bought neither).他看了两支笔,但一支也没有 买。 定语 You may take either book (=take one of the two books). =You can’t take both of the two books. 两本书你可以任选一本。 all 最少 表示 三个 以上 (肯 定) 主语All of them are workers.他们都是工人。 宾语 The teacher asked us all about the matter. 老师问了我们所有的事。 表语That’s all for today.今天就到这。 定语All men are mortal.人总是要死的。 状语He was all covered with mud.他浑身是泥。 同位语They all came here.他们都到了。 注: 1. all与定冠词、指示代词、物主代词连用时要放在它们的前面。 如: Do you see all the birds in the tree?你看到树上所有 的鸟吗? 2. all用作状语时,应放在实义动词之前,助动词之后。 如:The books were all sold out.所有的书都卖完了。 3. not与all连用时表示部分否定。 none (与最少 表示 三个 主语 None of them have come back yet.他们一个都还没有回 来。 宾语She chose none but the best.她只挑了最好的东西。
一、表格的用法 1.doing 的用法 (1)在要求动词后(作宾语):avoid避免appreciate 感激/欣赏acknowledge承认/自认 admit 承认advocate提倡/主张consider 考虑 can't help不禁 can't stand受不了contemplate细想complete完成confess坦白 dislike不喜欢,讨厌deserve值得 delay 延迟 deny否认 dread可怕defer拖延detest嫌恶 enjoy享有/喜爱envy嫉妒endure忍受excuse借口escape逃跑/逃避finish完成forgive原谅 fancy幻想/爱好favor 造成/偏爱figure描绘/计算hate讨厌 imagine设想involve卷入/包含keep保持miss错过mention说到/讲到mind 介意pardon原谅/饶恕permit允许 postpone推迟practice 实行/实践prevent阻止quit放弃停止risk冒险recall回想resist抵抗/阻止 resume恢复repent悔悟resent怨恨stand坚持/忍受suggest建议save营救/储蓄tolerate忍受
worth值得 You should try to avoid making mistakes. The book is worth reading. The book deserves reading. (2)表进行 Walking on the grassland, I saw a snake.=When I was walking on the grassland, I saw a snake. The man speaking English is Tom. = The man who is speaking English is Tom. (3)表主动 The man speaking English is Tom = The man who speaks English is Tom. = The man who spoke English is Tom. Nobody dinks boiling water but boiled water.= Nobody dinks water that is boiling but the water that has boiled. (4)表伴随 I stand outside waiting for Mr. Chen. I lie in bed reading a novel. (5)表性质;特点 The film is very moving. She is understanding, so you had better discuss your business with her.
Population用法 population是一个集合名词(无复数形式),它的用法有时较为特殊,所以很容易用错。 下面谈一下它的用法: 一、population常与定冠词the连用,作主语用时,谓语动词常用第三人称单数形式。 例如: The world\'s population is increasing faster and faster. 全世界的人口增长得越来越快。 At the beginning of the twentieth century, the world\'s population was about 1,700 million. 在二十世纪初,全世界的人口大约是十七亿。 二、当主语是表示\"人口的百分之几、几分之几\"时,谓语动词用复数形式。 例如: About seventy percent of the population in China are farmers. 中国大约有百分之七十的人口是农民。 三、有时population可用作可数名词,其前可用不定冠词。 例如: China has a population of about 1.3 billion. (=There is a population of about 1.3 billion in China.) 中国大约有十三亿人口。 New York is a big city with a population of over 10 million. 纽约是一个有一千多万人口的大城市。 在表示多个地区的人口时,population要用复数形式populations。 例如: Many parts of the world, which once had large populations and produced plenty of crops, have become deserts. 世界上很多地区一度人口众多,种植大量的农作物;现在,这些地区已经变成了沙漠。 四、表示人口的\"多\"或\"少\",不用\"much\"或\"little\",而要用\"large\"或\"small\"。 例如: India has a large population. 印度人口众多。 Singapore has a small population. 新加坡人口少。 五、询问某国、某地有多少人口时,不用\"How much...?\",而用\"How large...?\";在问具体人口时用\"What...?\" 例如: -How large is the population of your hometown? 你们家乡有多少人口? -The population of our hometown is nearly twice as large as that of yours. 我们家乡的人口是你们家乡人口的将近两倍。 -What is the population of Canada? 加拿大的人口有多少? -The population of Canada is about 29 million. 加拿大的人口大约有二千九百万。 六、population还表示\"某地、某类的动、植物或物品的总数\"。 例如: In India, however, the population of tigers has increased, from 2,000 in 1972 to about 5,000 in 1989. 然而在印度,老虎的总数已从1972年的2,000只增长到了1989年的大约5,000只。