Related Classifications
Hospice Facilities
Hospitals - General Care
Nursing Homes
Pharmacies
Rehabilitation Facilities - Physical Restoration
Special Exposures
Administration of drugs
Lifting residents or heavy items
Pets
Pools, whirlpools, and exercise equipment
Privacy
Substandard facilities of care
Unqualified personnel
RISK DESCRIPTION
A rapidly growing segment of the United States population is the elderly. In 1996, there were 34 million people over the age of 65, representing 13% of the nation's total population. By the year 2020, this age group is projected to nearly double in number and account for 20% of the total population. This increase has produced a large and growing number of senior citizens requiring medical oversight and formalized care. Assisted living facilities are designed to meet these increasing demands. These facilities combine the advantages of independent housing, supportive services, and social activities. They offer individual apartments or rooms, meals, housekeeping and laundry services, transportation, assi stance with basic activities of daily living (ADLs) and instrumental activities of daily living (e.g., bathing, eating), along with ongoing health and activity supervision.
Assisted living is an umbrella term for a wide range of new living settings where nursing home-eligible people live and receive care. However, while some persons may refer to assisted living facilities as nursing homes, they are not similar types of facilities; they offer different services, often to a different population. While both facilities offer medical services, nursing homes are designed to provide long-term health care and social services to the elderly, chronically ill, or convalescent persons. Assisted living facilities are designed specifically for elderly citizens, whereas nursing homes may house both elderly and young persons (i.e., those with chronic medical problems or severely injured individuals who are in need of 24-hour care). The goal of nursing home care is to provide care and treatment to restore and maintain the patient's highest level of physical, mental, and social well-being by providing round-the- clock health care services. The goal of assisted living is to help individuals live as independently as possible. This classification will focus solely on assi sted living facilities. For more in formation on nursing home care, refer to the Nursing Homes classification.
Currently, assisted living facilities are state regulated. Facility providers are chosen to work with state agencies to help establish quality standard, measurement, and monitoring approaches. Each of the 50 state departments of social services or public health responsible for licensing assisted living facilities has
different parameters and restrictions, as well as different names for the residences. Currently, there are 26 different terms commonly used throughout the United States, including such designations as residential care, personal care, boarding facilities, catered living, retirement homes, homes for adults, and adult congregate living care. While these various facilities may be referred to as assisted living facilities, each often offers its own unique type of services. The majority of states have existing licensing regulations using the term "assisted living"; for the purposes of this classification, all such residences will be referred to as assisted living facilities.
In 1996, people reaching the age of 65 had an average life expectancy of 82.7 years, which is 3.4 years more than their expectancy in 1960. While such recent medical advances as new medicatio ns, surgeries, and life-sustaining equipment have extended the human life span, an increase in the elderly population has brought forth a need for a disproportionately large share of medical services and assistance with daily activities. According to the U.S. Administration on Aging, daily living activities include eating, getting around in one's home, dressing, and bathing oneself. These older individuals sometimes need help with ADLs, and assisted living facilities are designed to provide the necess ary support.
Diseases related to dementia (i.e., ailments that affect the brain and alter memory, thinking, and actions, such as Alzheimer's disease) have affected life expectancies, and those suffering from such illnesses require the sort of increased care that assisted living facilities offer. Other factors contributing to the growth of such facilities include the fact that older persons now have higher incomes (over 53% of the U.S. elderly have incomes topping $15,000 a year and nearly 35% have an annual income of $25,000) allowing individuals to afford living in these residences; and the emergence of managed care and integrated delivery health care systems. Additionally, with more women entering the workforce, the number of family members able to care for aging relatives has decreased. It is estimated that more than 25% of seniors do not have relatives to whom they can turn for support in their later years.
Assisted living facilities debuted in the U.S. in the 1980s. These institutions were patterned after Dutch and Scandinavian systems egularly by the facility, and as the resident's condition indicates. The resident, his or her family, or another party responsible for the resident, play a role in the service plan's development by aiding the facility's personnel in determining what types of services and level of care the resident needs.
The resident may be placed in a particular level of care, if the facility offers such di stinct tiers. Examples
of these care tiers may include a level of minimal assistance where residents are only given direction on activities, meals, and medications; a stand-by assistance level where they are provided minimal hands-on assistance with dressing, 24-hour care, medications, meals, and direction on activities; and a hands-on assistance level where they receive aid in activities of daily living, help with incontinent care, diabetic monitoring, plus all other assi stance from the previously-mentioned levels.
Assisted living facilities typically do not provide continuous skilled nursing care. The facility should assure that prompt and appropriate medical, health, and dental care services are administered when required. The health care of each resident is under the supervision of the resident's chosen ph ysician. Residents suffering from temporary incapacity due to illness, injury, or recuperation from surgery may be allowed to remain in the facility if appropriate services can be provided or be readmitted to a hospital, if necessary.
Many elderly citizens are turning to assisted living facilities because they find them more appropriate and cost-efficient than other residences or facilities for the elderly, such as nursing homes or adult daycares. Compared to conventional nursing home care, assisted living facilities are 20% to 30% less expensive. More than 90% of the sector's revenues are generated from private pay. In 1998, assisted living facilities comprised a nearly $17 billion industry, which is projected to climb to over $23 billion by the year 2000. National expenditures for skilled nursing and home health care increased from $36 billion in 1985 to $106 billion in 1995 - expenditures that accounted for 11% of all health care costs in the U.S. Assisted living facilities offer the appropriate level of care for seniors at 25% to 50% less than the cost of a skilled nursing facility.
Assisted living facility costs vary greatly, depending on the type of residence, room size, and types of services required by residents. Private funds pay for 90% of assisted living services; the remaining 10% are covered by Supplemental Security Income (SSI), Social Security Block Grants, and other entitlement programs. In addition, several private health and long-term care insurance policies include assisted
living/residential care coverage. In 1998, 35 states reimbursed, or planned to reimburse, services in assisted living or board-and-care facilities as a Medicaid service. According to the American Health Care Association, 42% of all facilities receive state program assistance for residents. Currently, many states are
experimenting with expanding assisted living to low-income seniors through waivers to the federal Medicaid program.
The typical profile of an assisted living resident is a senior aged 75 or older (the average age for women is 84 and for men is 81) who meets the entry criteria of having at least $25,000 in annual net income, no combative or disruptive behaviors, and the ability to pay monthly housing rental fees of $2,000 or more. The average per-diem rate for the industry is $72; it is approximately $91 for residents in an Alzheimer's disease facility. Assisted living costs range from between $985 and $1,500 per month to $3,700 per month for a private 2-bedroom suite with minimal to moderate levels of personal care. Residents generally have personal assets ranging from $100,000 to nearly $300,000.
Conversely, as needs change, elderly people may relocate from assisted living residences. According to the National Center for Assisted Living, the majority of residents leave facilities because they are in need of a higher level of medical care. In 1998, the following were leading reasons why residents moved out of assisted living facilities: 43% went to a nursing facility; 22% died; 13% returned to their homes; 11% went to a hospital; 9% relocated to another assisted living residence; and 3% went to other settings. The average length of stay for an assisted living facility resident is three years.
Consolidation of assisted living facilities is one reason for the industry's increase. This continuing trend is a result of dominant companies (e.g., hotel chains and major corporations) seeking to strengthen their presence in specific geographic regions. Most of these acqui sitions have been for individual properties and small clusters of properties. Recently, however, there has been a growing number of acquisitions of entire public assisted living companies. The majority of the largest multi-facility providers are publicly held and managed as for-profit businesses. In 1997, 54% of assisted living facilities were part of a larger multi-facility organization with 10 or more residences; 25% were part of multi-facility organizations of 2 to 9 facilities; and 20% were single or stand-alone facilities. According to the Assisted Living Federation of America, in 1996, 85% of assisted living residences were for-profit, while 15% were not-for-profit facilities.
Assisted living facilities are located in rural, suburban, and urban areas in all 50 states. Facility developers have identified several locations as the highest selected regions due to favorable demographics and the relative absence of regulatory impediments in those states. In addition to the District of Columbia, these regions include: Florida, Texas, New Jersey, Pennsylvania, California, North Carolina, Washington, and Ohio. Most assisted living facilities are freestanding; however, they may also be part of a continuing-care retirement community, seniors' apartment co mplex, or wing or floor of a nursing home. The facilities may also be renovated schools or converted hotels, motels, or nursing homes. Facilities vary in terms of size. The average size of an assisted living residence is 43 units; however, facilities may range from 3 units to over 200 individual living quarters. The average number of residents in a facility is 40; however, small, homelike facilities typically house 3 to 12 residents, while large, full-service communities may accommodate 600 to 800 persons.
Assisted living facilities generally consist of a lobby, kitchen, administrative offices, medical and treatment areas, a common dining room, employee lounges, restrooms, and a parking lot. Common areas may include sun porches, a veranda, a library, a billiards room, television rooms, gardens, a beauty
parlor/barber shop, and fitness rooms. Individual units or shared rooms may be clustered in groupings of six to eight, and they vary in size from one room to a full apartment. Full apartments generally contain a bedroom, bath, closets, and kitchenette. These units often open in a suite-like fashion into a common sitting area or small living room.
Assisted living facilities generally operate 24 hours a day, 7 days a week; however, administrative offices are typically open from 9 a.m. to 5 p.m., Monday through Friday. Most facilities place no restrictions on visitors, who are generally allowed on the premises at any time. In addition, many insureds also allow residents to have overnight guests.
The number of personnel employed by assisted living facilities varies, depending on the size of the organization. Some states have requirements as to the number of staff needed in the facilities. For example, Alabama requires that there be one staff member per six residents in assisted living facilities at all times. Typically, a facility may hire anywhere from 10 to over 50 employees, including administrators, nurses, direct care staff (e.g., certified nursing assistants, certified home health as sistants), food service personnel, therapy consultants, activities coordinators, dietary consultants/dietitians, clerical staff, billing personnel, and housekeeping and maintenance workers. The ages of the workers vary; some may be as young as 16, while others may be over the age of 65. Some facilities hire temporary or part-time employees, such as students, during the summer; others have volunteers who assi st personnel and aid residents in such areas
as writing letters, reading, and providing companionship.
While assisted living facilities continue to prosper, there are several primary concerns that plague the industry: licensing delays, scarcity of trained employees, overbuilding in selected markets, and the inability to manage costs. Assisted living organizations and associations and the facilities' states are working to combat these problems by establishing new regulations and re- evaluating and creating new insurance and cost structures.
The assisted living industry, which is still a relatively new sector of elderly care, is anticipated to continue to grow as a viable alternative for long-term care. Factors that will aid in this upsurge include the continued number of people living to age 85 and over, elderly persons seeking appealing alte rnatives to inappropriate nursing home placement (e.g., being placed in a nursing home facility when they did not require that type of care), and government agencies recognizing these lifestyle trends and the possibility that they will introduce entitle ment programs to allow older people to choose a preferred assisted living setting. To provide future services to all elderly regardless of income, several states - including Connecticut, Illinois, Louisiana, and Rhode Island - are currently establishing pilot programs to address low-income residents' needs.
Several associations serve the industry. The organizations include the Assi sted Living Federation of America (ALFA, which may be reached at https://www.doczj.com/doc/ac11853147.html,), which is the largest trade association exclusively devoted to the assisted living industry and the population it serves. Other associations devoted to these facilities include the American Association of Homes and Services for the Aging (AAHSA, which may be reached at https://www.doczj.com/doc/ac11853147.html,) and the American Health Care Association (AHCA, which may be reached at https://www.doczj.com/doc/ac11853147.html,).
MATERIALS AND EQUIPMENT
Medical equipment and supplies, rehabilitative, and laboratory equipment; hospital beds; stretchers, wheelchairs and other walking aids; bathing equipment; first aid kits; wander-guard sensors (i.e., to keep dementia patients within the facility's premises).
Pharmaceuticals, including oral medications, subcutaneous injections (e.g., the vitamin B12, insulin),
eye/ear/nose drops, topical creams and ointments, suppositories/enemas, inhalers, etc.
Dietary and laundry equipment; housekeeping, cleaning, and maintenance equipment; recreational facilities and equipment; arts and crafts supplies.
Furnishings: tables, chairs, couches, televisions, VCRs.
Computer hardware and software; fax machines, copy machines.
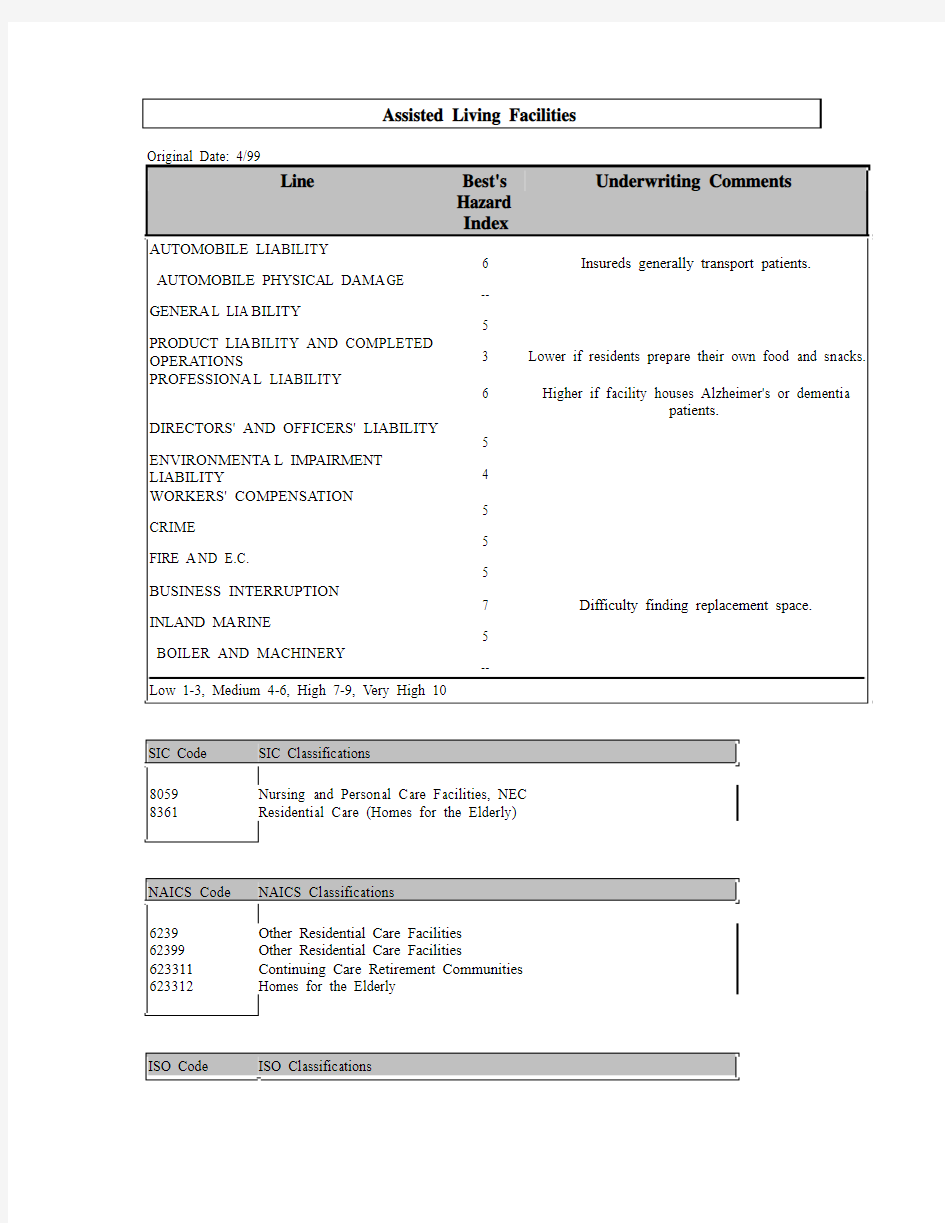
Automobile Liability
Because the majority of assisted living facilities will frequently transport residents to and from various locations, the Automobile Liability exposure will be significant. These facilities often transport residents to doctors' appointments, shopping malls, grocery stores, pharmacies, restaurants, theaters, libraries, and various other locations. Most facilities will have at least one vehicle to transport residents, although larger insureds may have a small fleet of vehicles. Assisted living facilities may also own cars, vans, or pickup trucks to run errands or get supplies. However, some facilities may require employees to use personal vehicles for business use, which would increase the exposure for this liability. Depending on the circumstances, travel may be done at night, when there is low visibility and drivers may be tired.
What are the frequency of travel, the radius of operations, and the hazards of typical routes? Most deliveries, pick-ups, and resident transports will be intermediate. Determine whether company-owned vehicles are used only to pick up supplies and run errands or are used to transport residents to and from facility-sponsored activities or off-premises locations (e.g., shopping malls, grocery stores, doctors' offices, and places of worship). According to the National Center for Assisted Living, the typical assisted living facility generates 1.73 trips per resident unit each day, as compared to 9.57 trips for the average single-family detached house and 6.59 trips for a low-rise apartment. What is the frequency of trips and destinations made by the insured and his or her employees? Routes to field trips may be unfamiliar t o the driver and may involve substandard or unpaved roads, or travel in high traffic, congested urban areas. Drivers may sometimes be required to operate vehicles before and after daylight, especially during the winter months. Darkness may result in decreased visibility, and at such times, drivers may be operating vehicles while they are fatigued. In addition, darkness may impede residents' visibility when boarding and
exiting vehicles. Are the insured's drivers required to operate vehicles while it is dark?
Does the insured operate a fleet of vehicles? Are the vehicles owned or leased? In some cases, insureds do not own buses but rather charter them for specific trips or tours. If so, determine the reputation of the bus company normally used by the insured.
Are safety restraints (e.g., seatbelts) used for all occupants? Are vehicles wheelchair-accessible? Due to various ailments and their frail nature, older people are more susceptible to injury in the event of an accident. Are residents assisted on and off the vehicle? Because accidents may occur during the loading or unloading of supplies or passengers, it is recommended that Automobile Liability and General Liability coverages be written by the same company for the same limits.
What are the number, age, type, and condition of the insured's vehicles? Owned or leased automobiles, vans, and buses may be used to run errands, to pick up supplies, and transport residents. Do employees ever take the insured's vehicles home at night or on the weekends? Occasionally, staff members may be called on to use their own vehicles. If employees use personal vehicles to run errands or transport residents, a nonowned vehicle exposure may exist.
What are the number, age, training, and experience of the insured's drivers? Does the facility transport clients, or do outside contractors provide transport services? Transporting elderly or disabled adults requires stable and experienced drivers. Does the insured have a safe-driver training program in place? An employee may be called upon to drive in an emergency; motor vehicle records should be obtained on all employees who are licensed drivers. Some facilities employ workers under the age of 25; a youthful operator exposure may exist. Request certificates of insurance from all drivers. Since the Fair Credit Reporting Act requires written permission from the driver to obtain MVRs, the insured should make obtaining this permission a part of the hiring process. Although infrequent, some facilities' drivers may operate oversized vehicles, such as buses or trucks. Operators of oversized autos will need the training necessary to drive these vehicles. A commercial driver's license (CDL) may be required to operate the oversized vehicles.
Does the insured have a vehicle maintenance program? The insured's vehicles should be kept in good condition, repaired promptly as needed, and inspected regularly. It is a positive underwriting sign if the insured contracts out vehicle maintenance to experienced mechanics. Employees should not be permitted to repair or assist in the repair of the insured's vehicles.
General Liability
Staff competence, the condition of the premises and equipment, and the physical layout of the building all affect the potential for injury. Many insureds will have a large number of visitors to their facilities daily. Primary premises exposures will be slips, trips, and falls. Additionally, some insureds may have volunteers working on site; this will increase the General Liability exposure. Because of the lack of uniform federal standards governing assisted living facilities, it is important for the underwriter to ascertain the standards (e.g., space and living quarter requirements) established by the state or county in which the facility is located and the degree to which these standards are adhered to by the insured's facility. Overall, assisted living facilities will have a moderate exposure in this line.
What is the layout of the insured's premises? The majority of fac ilities are freestanding; however, they may also be part of a continuing-care retirement community, seniors' apartment complex, or wing or floor of a nursing home. Assisted living facilities generally consist of a lobby, kitchen, administrative offices, a common dining hall, employee lounges, medical and treatment areas, restrooms, and a parking lot. Common areas may include sun porches, a veranda, a library, a billiards room, a television room, gardens, a beauty parlor/barber shop, and fitness rooms. Individual units or shared rooms may be clustered in groupings of six to eight, and they vary in size from one room to a full apartment. Full apartments generally contain a bedroom, bathrooms, closets, and kitchenette. These units often open in a suit e-like fashion into a common sitting area or s mall living room. Is the insured's facility owned or leased?
States have established requirements as to the space and type of living quarters for assisted living facilities. These resident unit requirements generally specify the minimum square footage, maximum number of individuals per unit, the areas or rooms to be included in each living quarter, and requirements for semi-private units. However, these requirements vary greatly from state to state. What are the insured's state requirements?
What are the insured's hours of operation? Assisted living facilities generally operate 24 hours a day, 7 days a week. However, administrative offices are typically open from 9 a.m. to 5 p.m., Monday through
Friday.
What are the average and maximum numbers of daily visitors to the insured's premises? Most facilities place no restrictions on visitors, who are generally allowed on the premises at any time. In addition, many insureds also allow residents to have overnight guests. What is the insured's visitation policy? Visitors to the site will usually include family members, clergy, delivery personnel, maintenance workers, inspectors (e.g., local building and health inspectors), guest speakers, and crafts/activities instructors. Does the insured offer tours (e.g., to potential clients, outside groups, or organizations) of the facility? An employee should accompany tour groups at all times. "Employees Only" signs should be posted in areas restricted to both visitors and residents. In some facilities, volunteers assist residents in writing letters, reading to them, or visiting them on a regular basis. Does the insured have volunteers who work in the facility and/or visit with residents? In some facilities, local clubs or social groups provide occasional entertainment or other services for the residents. Determine if such groups visit the insured's facility. Does an employee accompany the groups' members at all times while they are on the premises?
For visitors to the insured's premises, slips, trips, and falls will present the main General Liability exposure. What is the level of housekeeping on the insured's premises? The facility should be kept free of debris and clutter. Are residents allowed to empty their own trash into appropriately marked garbage containers located inside or outside the building? Trash and debris should be removed from the facility's premises on a daily basis. What is the condition of the insured's flooring? Floors should be swept and vacuumed on a daily basis. Worn, torn, or loose floor coverings should be repaired and replaced immediately. Spills should be cleaned up immediately, and "Caution - Wet Floors" signs di splayed. All electric wiring should be properly insulated and run inside the walls.
Does the insured comply with the provisions of the Americans with Disabilities Act (ADA) of 1992? This law requires that public buildings be wheelchair-accessible; restrooms and other areas of the facility must be readily accessible by wheelchair or other conveyances that assist di sabled or elderly residents. Since senior citizens and physically challenged residents may be hampered by the use of walkers, crutches, and wheelchairs, are emergency exit doors located throughout the premises? Are their locations indicated by signs clearly visible to residents and visitors? Stairs can be difficult for some elderly individuals to negotiate. Stairs should be in good condition, covered with a nonskid material, and equipped with sturdy handrails. Is the facility all on one level, or are there multiple levels? In most cases, a multi-level facility will require an elevator to assist seniors in moving from one level to the next. Who services the insured's elevators and how frequently? Generally, insureds will contract out elevator maintenance. Determine the reputation and loss history of the insured's elevator maintenance contractor.
Safety equipment should be installed or be available if needed in residents' bathrooms. This equipment may include grab bars, raised toilet seats, and seats in showers. Is safety equipment installed in the residents' bathrooms? Residents' living quarters should be equipped with emergency call systems linking the residents' units to nursing stations or other staff member locales. Is the insured's facility equipped with such systems?
The privacy of residents is a crucial element to these facilities. Privacy is primarily measured by the type
of unit, the ability of residents to lock their doors, and the staff's behavior. States that have based their policy on privacy have emphasized apartments with attached baths. When common or dormitory style bedrooms are provided, there should be a separation by partitions or screens to provide for privacy in ba th and toilet areas. As of 1998, 31 states had rules that allowed 2 people to share a unit or bedroom, and 11 of these states allowed sharing of units only by choice of the residents. What is the insured's state policy regarding privacy? Are two people allowed to share a unit or bedroom in the insured's state?
Most congregate assisted living facilities will have laundry facilities, unless commercial laundry services are used. Laundering facilities should be located in a specifically designated area. Insureds should prohibit visitors and residents from laundry areas because the chance of injury is increased as these individuals could be exposed to injuries from machinery and toxic cleaning solvents (e.g., detergents). Does the insured's facility have adequate room and space for sorting, processing, and storage of soiled materials? Provisions should be made for proper mechanical ventilation of the laundry, and adequate and effective lint traps should be provided for dryers.
Kitchens contain further potential for injury. The facility's kitchen should be separate from areas occupied by residents. Kitchen appliances may present a variety of hazards. For example, stoves may have open flames, while ovens may cause burns if residents reach over heated burners. The insured should restrict access to the kitchen to staff and kitchen employees only. Is the insured in compliance with local and state codes regulating kitchen and food preparation/serving areas? Many resident apartments/rooms contain a
kitchen or s mall "tea kitchen" (i.e., a kitchenette that contains a sink and refrigerator). Are residents' individual units equipped with kitchens? If so, the same hazards found in the facility's kitchen may also occur in residents' kitchens. Many resident kitchens have microwaves and/or hot plates. Do the insured's resident units have such appliances? If so, residents should be instructed how to properly operate these appliances. Injuries, such as strains, sprains, or falls, may result when residents reach for items in kitchen cabinets or shelves. If shelves are located too high off the ground, residents may climb onto chairs, potentially causing injury if chairs topple over or residents fall off them. Are cupboards and shelves in kitchen areas easily accessible so that residents do not have to climb or stretch to reach them?
Assisted living facilities often have microwave ovens on the premises in both the kitchen and residential units. Microwave rays present a danger to residents and workers with certain heart conditions who wear pacemakers. Does the insured post signs in kitchen areas that warn residents and employees that microwaves are being used?
Does the insured employ dietitians to assist residents who have special dietary needs (e.g., d iabetics)? Many assisted living facilities employ these individuals to prepare special dietary menus and requirements for patients who need specially prepared foods, such as no-salt diets and foods without sugar. Do dietitians instruct food preparation employees of any dietary needs? Are these specially prepared foods offered daily to residents with these requirements?
Does the insured have a pool on the premises? If the facility has a pool, particularly an in-ground pool or one that is a permanent structure and cannot be drained daily, the likelihood of a resident or visitor drowning will increase. A pool alarm should be used to alert staff if someone has fallen into the pool. What pool safety measures does the insured have in place? For example, an outdoor pool should be surrounded by a fence and have a locking gate installed on it to prevent access from outsiders. Does the insured employ a lifeguard? Staff should be trained in resuscitation techniques, and the insured should be in compliance with all state and local statutes regulating the operation of a public pool.
Medical research indicates that animals provide therapy to elderly and ailing persons. To meet these needs, along with providing companionship and enjoyment, some assisted living facilities allow residents to own pets (e.g., dogs, cats, or birds). According to the National Center for Assisted Living, nearly 50% of all facilities allow residents to keep small pets in their units or apartments. In addition, nearly 40% of all centers provide facility-owned pets for residents to enjoy. Does the insured's facility have its own pets? Are residents allowed to have pets in their living quarters or have pets brought to the facility by visitors? Some residents could develop an allergic reaction. Residents or visitors could be injured if not taught how to handle animals properly. Pets should be even-tempered and well-trained so they will not become agitated and bite, scratch, or claw residents or visitors. What is the level of supervision of these animals? All animals on the premises should be domesticated and non- aggressive, licensed and vaccinated, free from disease, effectively controlled, and prohibited from food preparation areas. What is the insured's practice?
Often, assisted living facilities will have artwork and decorative pieces (e.g., sculptures) displayed throughout the premises; some of the work hangs on walls and ceilings. This artwork could potentially fall and injure residents, visitors, or employees. How are decorative pieces secured to prevent them from falling?
Many facilities have large panes of glass both inside and outside (e.g., sliding glass doors, French windows). Glass should be properly etched or marked to prevent residents or visitors from walk ing into the clear glass.
What are the age, type, and condition of the insured's furnishings? Generally, residents bring their own furnishings for their living units. However, facilities will house a large number of furnishings, ranging from couches in lobbies and television rooms, to tables and chairs in recreation and dining areas. Furniture should be sturdy, free of splinters, and have no protruding nails or screws. Chairs, particularly those that swivel or rock, should be properly assembled and in good repair. What is the insured's practice of inspecting furnishings? The underwriter should evaluate the layout and condition of areas that contain seating furnishings (e.g., dining areas, recreation rooms). Is there adequate space between tables to allow residents to move comfortably and maneuver wheelchairs and walkers? In facilities where employees serve food to residents in dining rooms, there should be adequate space between tables to allow the servers to move freely. If tables are too crowded, the chance of a server dropping a hot plate on a resident may increase. Is there adequate space between tables in the insured's dining area?
In facilities that utilize servers in dining rooms, burns and cuts are potential hazards to residents. Thes e employees may spill hot dishes or beverages on residents or visitors, causing burns or damaging their
clothing. Are servers instructed how to properly carry trays and dishes? Do they warn diners that plates are hot? Cuts can be caused by broken glass or chipped dishware. Are glasses and dishes inspected before being used?
A resident may choke on food while in the dining area. Are employees trained in the proper first aid methods? Designated employees should be trained in first aid and cardiopulmon ary resuscitation (CPR) techniques to provide medical assistance. Are first aid kits located throughout the facility? Is a first aid kit available in each medical room or treatment area?
Does the insured have an on-site physical therapy and/or exercise facility? These areas typically contain various fitness equipment, such as exercise bicycles, treadmills, whirlpools, and walking assistance apparatus (e.g., parallel bars). Is the insured's equipment in proper working order? Who is responsible for inspecting, maintaining, and repairing the equipment? An employee (e.g., physical therapist or therapy assistant) should be present at all times when residents are using physical therapy equipment, as they can fall or potentially suffer a heart attack from misuse or overuse of the equipment. Are employees present when residents use whirlpools? At what temperature are the insured's whirlpools set and maintained?
The insured may be liable for use of faulty medical equipment. Determine the reputation of th e insured's medical suppliers. Are new staff members trained in the proper use of equipment? Does the insured have an ongoing maintenance program, in accordance with the manufacturers' specifications?
Most states require persons to sign agreements or contracts prior to becoming residents of a facility. The scope of the agreement varies but usually includes provisions dealing with services, resident rights and responsibilities, occupancy, and discharge issues. Do the insured's contracts stipulate info rmation on resident charges and fees? Most agreements include a description of the fee or charges to be paid, the basi s of the fee or what is covered, who is responsible for payment, and the method and time of payment. Refund policy may also be covered by these agreements. Rules covering contracts specify the amount of advance notice tenants must be given when rates are changed. Does the insured's service provisions describe the services to be provided that are covered by the basic fee and any additio nal services that might be available? Some states also require that agreements contain resident rights and the provisions that allow staff to inspect living quarters, with the residents' permission. Terms of occupancy may also address provision of furnishings and the policy concerning pets. Do the insured's contracts cover such provisions? Determine what the insured's state regulations require for service and resident contracts.
Does the insured secure the facility with enclosed patios and/or courtyards? Security issues are of great concern for elderly persons, particularly those with Alzheimer's disease and dementia, as these individuals often lose their reasoning and judgment and are easily disoriented. For example, a common characteristic of Alzheimer's disease is a compelling need to roam or wander in a seemingly aimless manner. Does the insured have a wander-guard alarm so staff will be alerted when someone leaves the building?
What is the condition of the insured's sidewalks and parking lots? Sidewalks and parking lots should be free of cracks and potholes that could cause seniors, physically challenged residents, and other visitors to the premises to slip and fall. Are snow and ice removed promptly? Does the insured or his or her employees remove snow and ice or is this service contracted out? Sidewalks and parking lots should be well lit.
Product Liability and Completed Operations
The Product Liability exposure for assisted living facilities will be slight. Most facilities will prepare and serve lunch, snacks, and beverages. The most serious exposure will be the possibility of serving clients tainted or spoiled food. If residents prepare their own meals and snacks, the Product Liability exposure will decrease.
Does the facility serve and prepare snacks, meals, and beverages? Is the food prepared by an outside professional food staff, by the center's staff, or by volunteers? Kitchen facilities should be clean, and all foods should be checked thoroughly before being prepared and cleaned if necessary. Is food stored properly? Storage containers should be properly marked and covered. Food is subject to spoilage or deterioration due to age, contamination, improper storage, or incorrect temperature controls.
How long has the insured been in business? What is the insured's financial condition? Financial problems can result in lower food quality and reduced maintenance/housekeeping standards, which will increase the chance of claims. Check the insured's financial records.
Good housekeeping is essential to control pests. How often are the premises sprayed for pests? The underwriter should check contracts made with pest control services. Other good housekeeping procedures
should be maintained throughout the kitchen and food preparation and storage areas. Floors should be swept and mopped daily. Garbage should be emptied daily, and containers should be washed and sanitized at the end of each shift.
Employees working in the kitchen should be properly trained to operate kitchen appliances and equipment, as well as to prepare food items. Has the kitchen been inspected and found to be satisfactory by the local health inspector? Are food and beverages stored separately from the cleaning supplies? Determine the reputation of the manufacturers of these food items and appliances, and the loss histories of these suppliers. Who is responsible for repair of broken or damaged appliances?
Proper food controls are important to prevent foodborne illnesses such as escherichia coli (E.coli) and salmonella. These diseases are caused when bacteria that live in the intestinal tracts of animals pass into meat and poultry when the animal is slaughtered; both cause severe diarrhea, fever, and abdominal cramps. Does the insured's food service prepare foods such as beef, poultry, and shellfish? The Centers for Disease Control and Prevention (CDC) and the U.S. Food and Drug Administration (FDA) have published strict guidelines regarding the storage and handling of these food products. These guidelines include that raw shellfish should be tagged with an FDA National Shellfish Safety Program tag, that raw foods should be separated from other food items and stored on a clean shelf space in the refrigerator, and that food should be delivered and stored at 41° F or below. For more information, see the Product Liability and Completed Operations section of the Restaurants classification.
Leftover food may become tainted if improperly stored and ideally should be discarded daily. Is a dequate refrigeration available? Perishables should be promptly refrigerated after use. Who is responsible for maintenance of the refrigeration units?
Proper room temperatures should be maintained in all food preparation areas. The FDA requires that a ll vapors and fumes be vented outside. Proper ventilation must be provided in hot food preparation areas, utensil washing areas, garbage areas, and toilet areas. Is the insured in compliance with OSHA standard 1926.57, Ventilation? All kitchen hoods should be approved by the National Fire Protection Association (NFPA) and should provide the proper amount of exhaust recycling in cubic feet per minute (cfm).
Does the facility use disposable plates and utensils for food service, or does it use plates an d utensils that require washing? Are dishes and utensils washed by hand or in a dishwasher? After rinsing, dishes should be sanitized with a bleach solution (e.g., one tablespoon per gallon of hot water). For a detailed discussion on proper dishwashing and sanitizing techniques, see the Product Liability and Completed Operations section of the Restaurants classification.
Allergic reactions to foods can also lead to claims. Are facility employees informed of the ingredients in
all menu items? Insureds may keep a binder with written ingredients in the kitchen area that employees can reference. What is the insured's practice? Some patrons may be strict vegetarians due to health or religious reasons. Are vegetarian dishes offered to residents? Many elderly persons also have special dietary requirements (e.g., diabetics who can only have regulated amounts of sugar). Do dietitians consult with food preparation workers about residents' diet requirements?
Are employees trained in proper hygiene methods? Does the insured post a policy regarding proper hygiene in the food area? Food prep workers should wear hairnets. In addition, food servers should wear their hair pulled back. Are employees instructed to wash their hands before handling food?
Is any merchandise or food sold in vending machines? If so, is a selection of food offered to accommodate patients with certain dietary restrictions (e.g., diabetics)? Ascertain the number and types of machines on the premises, the vendor's reputation, and whether any liability is assumed by the insured. For more information, refer to the Product Liability and Completed Operations section of the Vending and Amusement Machine Operators classification.
Professional Liability
The Professional Liability exposure assisted living facilities face will be significant. Exposures include insufficient licensing of personnel and the facility, negligent dispensing and administering of medications, and noncompliance with state specifications on the designated number of workers per residents. If the facility houses Alzheimer's or dementia patients, employees should be required to have additional training or the exposure for this liability will increase.
States license assisted living facilities. Since these facilities are generally less intensive than a skilled nursing home, assisted living facilities will typically have fewer licensing requirements; however, since they often provide more services than an independent living retirement community, they will require a
higher number of licenses than those residences. Is the insured's facility licensed by the state and in good standing? Is the facility Medicaid certified? There are several types of licenses that an assisted living facility might hold, including a standard license issued to provide basic support services; a limited nursing license that allows the facility to provide residents with more assistance and specified limited nursing services that may be defined by the Agency for Health Care Administration; a limited mental health license that provides for supervision and monitoring by specialized staff and individualized supportive services to meet the special needs of the resident; or an extended congregate care license that is designed to enable residents to "age in place" (otherwise, they might be disqualified from continued residency based on their level of care needs). "Aging in place" essentially is designed to protect patients from being removed from an assisted living facility as their need for additional services or medical treatment increases. What type of license does the insured's facility hold?
Does the facility have separate areas for caring for sick residents if they are unable to remain in their living quarters? Who administers medications and what are their experience, qualifications, and training? Claims commonly result from negligent dispensing and administration of drugs. Although some states require a licensed nurse to administer drugs and medications, many others require only that an employee receive some training in medication administration. All medications should be kept in a locked cabinet.
Does a physician prescribe all administered drugs, and are all prescriptions dispensed in accordance with written drug orders? Determine if the insured has a licensed pharmacy on the premises or an agreement with an outside licensed pharmacy or pharmacist consultant. Is the insured's pharmacist currently licensed by the state in which he or she practices? Determine the training, experience, and qualifications of the pharmacist or individuals who dispense and administer medications to residents.
Records of receipt and disposition of controlled drugs should be sufficiently detailed and accurate. What is the insured's system for recording drugs taken from the pharmacy or medication-dispensing area and administered to patients? The facility's medical personnel should be aware of any allergies residents might have. Are all adverse incidents regarding medications recorded and reported to a physician? The nursing staff should be periodically provided with refresher courses and new information on drug therapy.
Some medications and drugs must be stored in a specific temperature or in or out of the light (e.g., Diazepam, or valium, which is indicated to be stored between 15° and 30° C and kept in a tightly-closed, light-resistant container). Are all drugs stored under proper temperature, light, and security?
Is self-administration of medication allowed in the insured's facility? Most assisted living facilities allow residents to keep medications in their apartments or units. Are residents who self-medicate encouraged to have their medications reviewed by a health care professional at least annually or more often if necessary? Does the facility have policies and procedures that do not interfere with the rights of the resident, but protect the health and safety of other residents? For example, a resident may wander into the wrong room and take medicine that belongs to someone else.
Does the insured have any policies for prescription medications? Generally, prescription medications should have a pharmacy label that includes the resident's name, name of the medication, prescribed dosage, and directions for use. Medications should only be used for the resident identified on the pharmacy label. Does the insured keep stock of commonly used, over-the-counter medications? Does the insured dispose of medications after the death or eviction of a resident? It is a positive underwriting sign if insureds develop and follow a written policy for the disposition of unused, outdated, or recalled medications. Does the insured have such a policy in use?
A critical area of staffing for facilities is 24-hour awake staff to deal with residents suffering from dementia because many such persons are awake and active at night. Do facilities with these patients have staff available 24 hours a day? Staff members should be available not just for monitoring and supervision but also to provide individual attention and activities, even during the evening hours. Having staff to fill this need on a 24-hour basis both occupies the person with dementia and avoids disturbance of residents who are sleeping. What is the insured's practice for staff involved in the care of residents with dementia? What are the training, experience, and qualifications of professional services' employees? Most insureds and their employees have special training as a result of either state requirements or assis ted living residence policies. Some states require special staff certification and training. What is the experience of the insured's physicians, nurses, and other professionals on staff, and what are the privileging procedures for attending physicians? What are the insured's criteria for medical staff qualifications? Physicians must be properly licensed and certified. Nurses should have a bachelor's degree, associate degree, or certification from an accredited college, university, or nursing school. State requirements indicate the number of years of experience these individuals must have. Many insureds require that direct care staff be
certified nurses or home health aides. What is the insured's practice?
Most states require their facilities to have a certain number of staff members per residents. For example, in Georgia, an assisted living facility must have 1 staff person per 15 residents during working hours and 1 per 25 residents during nonworking hours. Determine the ratio of nurses to patients. Is the insured's number of staff sufficient to meet the needs of the residents?
State requirements vary as to the requirements of other staff members. Many states are adding requirements that staff in facilities serving Alzheimer's patients receive special training to respond to these patients' unique needs. For example, in Maine, all new employees in facilities with Alzheimer's/Dementia Care Units are required to receive a minimum of eight hours of classroom orientation and eight hours of clinical orientation. If the insured houses Alzheimer's patients, what are the employees' educational and training requirements?
Requirements for training new staff vary from state to state. The rights of residents is the most frequently cited area for required training. Most state regulations require an orientation for new staff and annual in-service training. What is the insured's practice for training new employees? Some states require direct care staff to successfully complete an approved course, while others specify the areas to be covered during training, the number of hours to be spent in training, and requirements for both topic areas and the number of hours. Training requirements may be grouped into five domains: direct care, health related, knowledge areas, safety and emergency issues, and process.
Have any of the insured's professional workers ever had complaints filed against them alleging professional misconduct? Elder abuse by caretakers at seniors' residence facilities have been reported in the media, and assisted living facilities must take every precaution to prevent claims of this type. Defending against these claims is expensive, even if the facility is later cleared of all charges. Charges of abuse can result from a staff membe r restraining or punishing an unruly resident. Does the facility forbid employees to engage in any type of corporal punishment? Are employees trained in the proper ways to restrain an unruly resident? The facility's discipline policy should be discussed with all caregivers and the residents themselves.
Does the insured perform criminal background checks on potential applicants? Some facilities perform a criminal check and Adult Abuse Registry check on employment applicants. Some states' legislation indicates that facilities should not employ or retain a worker who has had a substantiated charge, in any state, of abuse, neglect, or exploitation, or who has been convicted of an offense for actions relating to bodily injury, theft or misuse of funds or property, or other crimes inimical to the public welfare. Does the insured's state indicate such provisions? Insureds should retain records of any criminal and Adult Abuse Registry checks. What requirements must the insured follow to make reports to his or her state's Adult Abuse Registry?
Directors' and Officers' Liability
Assisted living facilities will have a moderate Directors' and Officers' Liability exposure. Possible exposures for this liability include insufficient continuing education requirements and mishandling of funds.
Does the insured have one or more administrators who oversee the facility's operations? Assisted living facilities generally have at least one administrator who is responsible for the overall operation of th e facility. He or she ensures that all staff members are qualified to care for the residents and are competent in performing their duties consi stent with applicable state and federal regulations. It is the administrator's duty to assure that each resident receives all services indicated in the resident's service plan. Administrators should be state licensed. In some states, administrators are required to complete a state-approved certification program. These requirements vary greatly from state to state. What are the insured's state requirements on certification of administrators? Additionally, many administrators annually accumulate continuing education units (CEUs) appropriate to the scope of services provided. These CEUs may be approved by the state's board of nursing facility administrators, board of nursing, board of social work, or other appropriate state agency.
Obtain a full disclosure of ownership and an annual operating budget and financial statement on the insured's facility. State licensure and federal certification reports are public records and should also be obtained. Does the insured maintain incident and accident report files? Determine if these report files are submitted to the proper authority as required.
Review the admin istrative policies and procedures concerning admissions, transfers, discharges, charges,
payments, safekeeping of residents' valuables, and handling of residents' personal and financial affairs. Do the insured's policies and procedures protect against allegations of the mishandling of resident funds; billing for deceased or discharged residents; double-billing; improperly assigning the cost of the owners' or administrators' personal items; kickbacks; billing for services not utilized by the patient; and other financial irregularities?
Environmental Impairment Liability
Assisted living facilities will have a minor Environmental Impairment Liability. Claims may arise from improper waste disposal and water temperatures. State and local agencies have regulations for air, water, and ground pollution control. These regulations should be checked to see which ones impact upon the insured's operation of his or her facility. If the insured has a medical laboratory area on-site, the exposure for this liability will increase.
Although rare, an assisted living facility may have a laboratory on the premises. Does the insured have an on-site laboratory area? Medical laboratories handle many hazardous and toxic chemicals. Does the insured follow Environmental Protection Agency (EPA) guidelines regarding the collection and disposal of waste chemicals? What is the volume of hazardous substances in laboratory areas? In most facilities, the amount of toxic chemicals kept in the laboratories is s mall enough to make a claim unlikely.
An assisted living facility's water supply should be taken from a water system that is protected, operated, and maintained in conformance with state and local regulations. Do the insured's state and/or local regulations indicate the maximum temperature for residents' units; for example, in Vermont, hot water for use in residents' units may not exceed 110° F. In addition, water temperatures in the central kitchen and laundry areas used for sanitizing should meet local and state health department standards. What is the insured's practice? Water that is unsafe for drinking should be appropriately labeled and segregated. Some facilities discharge their wastewater into municipal sewage systems. Wastes are compatible with municipal treatment facilities for the most part. However, the insured should establish in-process controls - such as mercury, barium, and silver collection procedures - to prevent the discharge of toxic, radioactive, or highly corrosive wastes. Is the insured's business connected to municipal treatment facilities? Facilities that are not so connected should treat their wastewater.
Potentially infectious or pathological wastes should be kept separate from other trash by means of colored containers and colored trash bags coverage. Some employees, such as physicians, social workers, and dietitians, may be available on call.
Employees may suffer various types of injuries, such as slips, trips, and falls. What is the level of housekeeping? Areas should be kept free of debris and clutter. Trash and debris should be removed from the premises on a daily basis. What is the condition of the insured's flooring? Floors should be swept and vacuumed every day. Worn, torn, or loose floor coverings should be repaired and replaced immediately. Spills should be cleaned up immediately, and "Caution - Wet Floor" signs displayed. Is there adequate aisle space between desks in office areas? Wiring and telephone cords should not be stretched across aisles or walkways.
Employees are subject to repetitive motion injuries, such as carpal tunnel syndrome, as a result of their use of computers, typewriters, and calculators. In addition, direct care personnel may suffer back injuries, including sprains, strains, dislocations, and hernias, resulting from lifting residents who may have fallen
or need assistance with getting out of bed. In addition, back injuries may result from maneuvering patients in wheelchairs (e.g., placing strain on the employee's back or muscles, or incorrectly turning their bodies to push or pull the chair). Lifting heavy objects may also cause these injuries. Does the insured instruct all employees in proper lifting techniques? Employees should be encouraged to obtain help before moving o r lifting residents and heavy items.
Service personnel (e.g., laundry, food service, maintenance) may experience other types of injuries, including cuts, burns, and eye and skin irritations. For employees who work in the food service area, cuts from kitchen equipment may be common. What is the layout of the kitchen, including the arrangement of the equipment? How are knives and other sharp objects stored? Burns from kitchen stoves and grills may also occur. Are employees trained in the proper use and safety of kitchen equipment?
In facilities where employees serve food to residents in dining areas, are servers trained how to properly carry trays and hot dishes? To accommodate a large number of residents, employees may be hurried as they deliver food to the tables. Are employees instructed to warn other employees when they are nearby with hot dishes or heavy trays? Burns can be prevented if cooks use padded mittens to handle pots.
Does the insured have a laundry operation on the premises? Laundry personnel may be exposed to lifting injuries, steam and hot water burns, iron burns, and irritating detergents. Floors are often wet and slippery in these areas; falls may be common. Are "Caution - Wet Floor" signs posted in laundry areas? Are spills, such as water puddles caused by washers, mopped up immediately?
Maintenance workers may be injured while making indoor repairs and while cleaning the facility areas. Falls and tool-related injuries are major exposures for these workers. Do the insured's employees make repairs to outdoor pools or grounds? Are they trained on proper safety precautions in these areas (e.g., not using electrical appliances or tools near water)?
Employees may be exposed to a variety of communicable diseases. Though less likely, employees may also be exposed to serious bloodborne pathogens, such as HIV and hepatitis B. Are employees advised to get a hepatitis B vaccination? Is the insured in compliance with OSHA standard 1910.1030, Bloodborne Pathogens? Handwashing is the most common preventive measure against the spread of communicable diseases. Are all employees required to wash their hands with soap and water before preparing and serving food, after using the restroom, after assisting a resident in the restroom, and after caring for a sick or injured person?
What kinds of personal protective equipment does the insured provide for employees for dealing with bloodborne pathogens and other infections? When there is occupational exposure, the insured should provide employees with appropriate personal protective equipment (e.g., gloves, gowns, laboratory coats, face shields or eye protection, mouthpieces, resuscitation bags or other ventilation devices). During normal use, this equipment should prevent blood or other potentially infectious fluids from reaching employees' work clothes, street clothes, undergarments, and skin, eyes, mouth, or mucous membranes. Is the insured in compliance with OSHA standards 1910.133, Eye and Face Protection, and 1910.134, Respiratory Protection?
Is the insured in compliance with OSHA standard 1910.138, Hand Protection? Gloves should be worn when it may be reasonably anticipated that an employee may have hand contact with blood or other potentially infectious fluid, or when handling or touching contaminated items or surfaces. Disposable, single-use gloves must be discarded as soon as their ability to act effectively has been compromised; disposable gloves must not be washed or otherwise reused. Hypoallergenic gloves, glove liners, powderless gloves, or other measures should be provided for employees who may be allergic to the gloves normally provided.
Although rare, an assisted living facility may house a medical laboratory area to process results or blood work on residents. Does the insured's facility have such an area? If so, employees working in a medical laboratory may be exposed to toxic, caustic, and acidic chemicals. What chemicals does the insured use and store? Containers of hazardous chemicals (e.g., acetone, benzene, ethyl alcohol) should be labeled clearly and contain appropriate warning statements. Are emergency overhead showers or hoses and eyewash fountains provided in case of an emergency? It is advisable that laboratory areas stock special spill kits, chemical antidotes, and first aid kits.
Are any pre-employment examinations done? Because some staff may be called upon to lift residents or heavy equipment, they will require physical strength and agility. A re the insured's physical exams designed to test individuals' strength and agility? Some facilities perform a his coverage typically includes clothing, personal effects (e.g., radios and televisions), and additional personal items. Money and securities are not covered.
Does the insured store prescription medications on the premises? All drugs and medications should be kept in a locked cabinet or closet with limited access to employees; daily inventories should be taken. Does the insured have a system for recording medication withdrawals? Determine the insured's security methods. Are personnel required to wear identification badges? If so, determine if these badges designate who has access to medications and drugs.
What type of security measures is taken by the insured to protect the premises? It is recommended that service areas (e.g., laundry, food service) be kept locked at all times. All exit doors should be equipped with double- cylinder, dead-bolt locks; windows should be equipped with tamperproof locks. Do residents have their own lockable doors in their units or apartments? Parking lots and sidewalks should be well lit. What type of alarm system does the insured have installed? Ideally, the insured's alarm system should be connected to a central-station alarm monitoring facility. What is the response time of the local police?
Fire and E.C.
There will be a moderate Fire and E.C. exposure for assisted living facilities. Primary ignition sources include inadequate wiring, s moking, kitchen and cooking equipment, laundry facilities, and malfunctioning electronic equipment. Reducing the ignition sources will minimize the potential for fires and explosions. The fire load for these facilities includes furnishings, cleaning materials, trash, and paper products.
What are the age, type, condition, construction, and layout of the insured's premises? The majority of facilities are freestanding; however, they may also be part of a continuing-care retirement community, seniors' apartment complex, or wing or floor of a nursing home. Facilities vary in terms of size. Typically, assisted living facilities range from 40 to 120 units. These businesses may be housed in converted buildings or in newly constructed facilities. The structure may be made of wood, brick, or masonry. Doe s the insured share a building with other facilities? Adjacent facilities should be separated by a firewall that extends to the ceiling. What are the hazards presented by nearby occupancies?
What is the layout of the premises? Assi sted living facilities generally consist of a lobby, kitchen, administrative offices, medical and treatment areas, a common dining hall, employee lounges, restrooms, and a parking lot. Common areas may include sun porches, a veranda, a library, a fully-equipped kitchen designed for food preparation or a warming kitchen where food can be kept at proper serving temperatures, administrative offices, a medical or first aid office, activity rooms, gardens, a library, TV rooms, a beauty parlor/barber shop, and fitness rooms. Individual units, apartments, or shared rooms may be clustered in groupings of six to eight, and they generally contain a bedroom, bath, closets, and kitchenette. They often open in a suite-like fashion into a common sitting area or s mall living room.
Ignition sources typically include electrical wiring, kitchen appliances, laundry equipment, electrical equipment, heating equipment, and chemicals (if a medical laboratory is present on the premises). In older buildings, heating equipment (e.g., gas or electric furnace) may be inadequate or in poor condition. Is the heating system regularly inspected and maintained by a qualified professional? A poorly maintained heating system could ignite nearby combustible materials and cause a fire to spread throu gh the whole building. Many resident apartments or units have individually controlled heating and air conditioning systems. What type of systems do the insured's resident units have in place? How often are these systems inspected and maintained?
What is the age, type, and condition of all electrical equipment used by the insured? Office areas may contain typewriters, computers, desk lights, and other equipment that may be electrically powered. Individual units and common areas may also contain electrical appliances (e.g., TVs, VCRs, stereos). In addition, some medical equipment (e.g., X-ray machines, treatment lamps) may be electrically powered. All electrical equipment should be in good repair, inspected regularly, and serviced by a licensed professional. What are the training, experience, and qualifications of persons who inspect and service the insured's electrical equipment?
Equipment requiring high voltage to operate is most susceptible to electrical loss and fire. If the insured operates out of a converted or renovated structure, check if any rewiring has been done and whether the new wiring is able to handle the insured's electrical needs. Wiring should be in compliance with NFPA 70, National Electrical Code. Is a planned program of scheduled inspection of all wiring and preventive maintenance by a qualified electrician conducted to reduce the possibilities of electrical accidents? Is a continuous power system or backup power source available?
Kitchen facilities will present additional ignition sources; for example, stoves, ovens, toasters, hot plates, and microwave ovens could overheat or ignite nearby combustibles, causing a fire. Does the insured have a kitchen or food warming area? W iring on all electrical appliances found in the kitchen should be inspected periodically for fraying and cracking. Are these appliances properly grounded and NRTL-listed? When in use, are kitchen appliances always supervised by an employee? The insured should designate an employee to make sure that all appliances have been turned off at the end of the day.
Storage of dry foodstuffs (e.g., flour) concentrates a high fuel loading in a relatively s mall area. Such items should be stored in covered metal bins.
Are cooking ranges protected with automatic extinguishing systems that cover both the grease producing surfaces and the exhaust ducts? Frequent cleaning of areas where grease buildup occurs is essential. Stoves should be equipped with hood and duct fire suppression systems that are inspected and cleaned regularly by a qualified contractor. Is the insured in compliance with all state and local ordinances regulating the operation of a commercial kitchen/food preparation area?
Laundry facilities contain both ignition sources and concentrations of combustibles (e.g., dryers). Malfunction of laundry equipment can cause fires that feed and spread rapidly due to accumulations of
linens. Are washers and dryers periodically serviced? The machines should be kept free of dust. Dryer exhaust ducts should be vacuumed or blown out frequently to prevent lint buildup. Is an automatic sprinkler provided at both ends of laundry chutes, at the top and in the receiving room?
Control of the storage and handling of flammable and combustible chemicals, particularly solvents, is a consideration if an assisted living facility houses a medical laboratory area. Are such chemicals stored on the premises? Unprotected gallon-size glass bottles of flammable solvents (e.g., acetone, methanol, and ethyl alcohol) are potentially dangerous. What is the insured's practice for storing and handling flammable and combustible chemicals?
Determine if the insured allows smoking on the premises. If s moking is permitted, is it restricted to certain areas? Are residents allowed to s moke in their rooms/apartments? "No Smoking" signs should be posted in all areas where smoking is prohibited. If smoking is permitted, ashtrays should be emptied into self-closing, fire-resistant containers. Where do residents dispose of smoking materials and ashes?
What are the average and maximum values exposed to loss? A typical assisted living facility will generally have many items of high value exposed to loss, such as medical equipment, whirlpools, audio/visual equipment, etc. Valuable papers and records, such as resident contracts and medical records, will be covered under Inland Marine; refer to the Inland Marine section of this classification for more information. What type of fire detection and suppression systems does the insured have in place? It is a positive underwriting sign if automatic sprinkler systems are installed in the structure. Is the insured in compliance with all fire codes? There should be a sufficient number of annually tagged and inspected Class ABC fi re extinguishers located throughout the premises, especially in kitchens, laundry areas, and resident units. These extinguishers should be used, placed, and maintained in accordance with NFPA 10, Standard on Portable Fire Extinguishers. Are extinguishers routinely serviced, and are employees trained in their use? Most facilities will be required by state and local building codes to have automatic sprinkler systems installed within the buildings and in individual living quarters. Does the insured hav e a sprinkler system in place in each resident's quarters? Determine if the insured has a sufficient number of smoke detectors in the facility and in each resident unit.
Does the insured maintain a written fire control and evacuation plan? These plans should be appropriately posted in each facility in a conspicuous place and kept up-to-date. Check the insured's state requirements on the number of fire drills that should be performed each year. For example, in Alabama, fire drills are required to be conducted at least 12 times per year, 4 times a year on each 8-hour shift. The drills may be announced to residents and employees in advance, and the drills should involve the actual evacuation of all residents to an assembly point as specified in the emergency plan and should provide residents with experience in exiting through all exits required by the state's code. What is the insured's practice?
Is the insured's business connected to a central-station alarm monitoring system? Instructions for fire emergencies, including emergency contact telephone numbers, should be clearly posted throughout the premises. Has the insured taken part in any pre-fire planning service? Determine the response time of the local fire service.
It is possible that a moral hazard may exist. How long has the insured been in business? Determine the facility's financial situation. The underwriter should examine the insured's financial statements for the last three to five years. What is the level of competition in the area?
Business Interruption
The Business Interruption exposure for assi sted living facilities will be substantial. If the insured operates a larger facility where many individuals reside, there may be difficulty in finding replacement space. Additionally, most insureds will likely choose to remain in the area where the previous center was located. Consequently, many insureds may choose to rebuild rather than to relocate.
Determine the time needed to rebuild or relocate; compliance with state governmental building standards may increase the time needed to rebuild. Since some of the residents may have no other place to reside (e.g., due to having sold a home to move into the facility), it may be difficult for them to seek immediate residence at another location. However, if they do seek residence at another facility, it may be difficult to attract those clients back to the insured's business once the facility has been rebuilt. Does the insured have an emergency backup plan in case the facility becomes unusable? Does the insured own or lease the premises? Depending on the severity of the damage to the premises, the facility may be operational while repairs are being done.
Relocation of patients may be necessary due to fire or related perils. Does the insured own another facility?
How long would it take to find nearby replacement space if the insured is unable to rebuild? Extra Expense coverage may be needed to cover the cost of renting an alternative facility. Insureds who decide to relocate will probably prefer to find replacement space in the vicinity of the original center to prevent the loss of most of their residents. Some insureds will have contingency plans in place prior to loss to ensure no interruption. What is the insured's practice?
Does the insured depend more on location or on reputation? As the number of elderly citizens continues to increase, the demand for assisted living facilities rises. Facilities are generally not dependent on specific locations, as the need for these facilities is nationwide. However, insureds may prefer to operate a facility somewhere that is more heavily populated, such as an urban or suburban area. According to the Assisted Living Federation of A merica, the location of an assisted living residence may determine the problems and challenges that the provider may experience. Urban locations tend to require higher
development/construction and labor costs while potentially providing, in the "right" location, a significant pool of income- and age-qualified residents. Suburban locations tend to require a strong sponsor/resident relationship where typically a parent is being moved closer to an adult child's family. A rural locale often results in lower development/construction costs and sometimes has less competition, but may require an operator to broaden his or her marketing to a larger geographic area in order to draw enough residents. What is the length of time needed to replace equipment? Ascertain whether medical equipment and supplies are easily replaceable. In general, most equipment and supplies typical of a standard assisted living facility will be readily available from local suppliers, and therefore, are not difficult to replace. However, some equipment, such as medical equipment, whirlpools, and audiovisual equipment, may be expensive to replace; this may increase the exposure. Loss of patients' records could cause a substantial delay in reopening. Does the insured have a policy on periodic backup of records?
Coverage for a loss of electrical power may be needed. In the event of a substantial power loss that cannot be restored by a backup system, the insured may have to make arrangements for relocating patients to other facilities. What is the insured's practice?
Inland Marine
There will be a moderate Inland Marine exposure for assisted living facilities. Insureds will likely require coverage for Goods in Transit, Electronic Data Processing (EDP), Accounts Receivable, and Valuable Papers and Records.
Medical equipment that is used off the insured's premises and during patient transportation may be scheduled. Coverage for wheelchairs, stretchers, walkers, and similar aids, as well as coverage for recreational, maintenance, and contractor-type equipment, may also be necessary. How do staff members keep track of medical and recreational equipment taken off the assisted living facility's premises? Are vehicles ever left unattended?
What is the age, type, and condition of the insured's computers? While many insureds choose to cover their data-processing equipment under a combination of Boiler and Machinery and Property policies, an Electronic Data Processing (EDP) policy may still be necessary. All computers should be etched with identification numbers to aid in their recovery if stolen. Does the insured use any custom-made software? Copies of all software and computer files should be stored off premises in an NRTL-listed, fire-resistant safe. Computer files should be backed up daily. Also, the facility may have office equipment and audiovisual equipment or cameras on the premises. If so, Property Floater coverage for these items may be necessary.
The insured may also wish to consider Valuable Papers and Records coverage for important documents such as records of daily transactions, financial statements, medical records, service and resident agreements and contracts, and licenses and facility-operating documents. Copies of these documents, along with billing records, endorsed checks, and other important records, should be kept in a fire-resistant, NRTL-listed safe off premises.
Outdoor signs may be subject to damage from wind and vandalism. If the insured has a sign, what is its type and condition? Is the sign freestanding or securely anchored to the building? A Neon Sign Floater may be necessary. Outdoor signs less than 12 feet above the sidewalk ordinarily are not acceptable.
Boiler and Machinery
Generally, assisted living facilities will have a slight Boiler and Machinery exposure. It will be greater for
larger insureds, but even so, the exposure will be more severe than frequent. Heating and air conditioning equipment will need coverage for breakdowns, as will refrigeration equipment required for food storage. What is the condition of the insured's heating and cooling systems? In older buildings, heating equipment (e.g., gas or electric furnace) may be inadequate or in poor condition. Is the heating system regularly inspected and maintained by a qualified professional? Many ass isted living facilities' resident apartments or units have individually controlled heating and air conditioning systems. What type of systems do the insured's resident units have in place? Breakdown of the insured's heating and/or air conditioning equipment could impair the facility's proper operations. In addition, breakdown could also result in illness or medically-related problems for residents, particularly because of their elderly and/or frail nature.
What are the age, type, and condition of the insured's refrigeration systems? Chlorofluorocarbons (CFCs) had been commonly used until the Clean A ir Act of 1990, which curtailed them. Since then, ammonia-based refrigerants have become a growing alternative to CFCs. These refrigerants are highly co mbustible and toxic. Is the insured's refrigeration system checked regularly for leakage? A mmonia-based refrigerants, along with other combustibles (e.g., certain cleaning solvents), should be kept away from ignition sources. If the facility experiences an electrical failure, food spoilage may occur. What are the values exposed to loss? Does the insured have a backup power source available in case of a power failure?
Assess the insured's boiler and cooling system maintenance and inspection programs. Who is responsible for inspecting and maintaining the system? What are their training, experience, and qualifications? Determine if boiler inspectors meet licensing requirements.
Underwriter's Checklist
Does the insured transport residents?
Are buses chartered for trips or tours? What are the bus companies' reputations?
What are the state requirements for the insured's resident living quarters?
What is the insured's visitation policy?
Is safety equipment installed or available if needed in residents' bathrooms?
Are laundry facilities located on the premises?
Does the insured's facility have a pool?
Who administers medications to residents? Are medications kept in a locked cabinet?
Does the facility serve and prepare snacks, meals, and beverages? What is the reputation of
manufacturers of food items?
Are potentially infectious or pathological wastes incinerated or autoclaved before disposal?
What are the professional qualifications of the facility's administrator(s) and staff?
Can the insured relocate in the event of a total loss, or can an alternate site be rented?
Do residents have their own lockable doors in their units or apartments?
Are fire drills conducted regularly under qualified supervision?
Risk Management and Insurance Chapter 1 Introduction to Risk 4. Differentiate between a peril(风险事件)and a hazard(风险因素)and give an example of each. (P9) A peril is a specific contingency(意外事件)that may cause loss. Examples of perils include fire, windstorm(暴风), collision(冲突), war, etc. A hazard is a condition or situation that makes it more likely that a peril will occur. Examples of hazards include oily rags(油布), icy roads, a dishonest employee, a careless driver, etc. Hazards include: ?Physical hazards(物质风险因素), like ice on the sidewalks, smoking, or skydiving; ?Moral hazards(道德风险因素)(most of which are avoidable), like dishonesty (such as burning down the warehouse(仓库)when your company goes bankrupt(破产)to collect insurance money or buying insurance on someone with yourself as beneficiary(受益人)and then killing them); ?Morale hazards(心理/行为风险因素), like a careless attitude since “insurance will pay for it” . 5. Classify each of the following hazards as physical, morale, or moral. (P9-10) a. A careless driver; b. A person who suffers an exaggerated(夸张的)case of whiplash(脖子扭伤)following an automobile accident; c. A worker who occasionally leaves a dangerous machine unattended to talk with friends; d.An employee who occasionally embezzles(挪用)money; e.Icy road conditions. a: Morale; b: Moral; c: Morale; d: Moral; e: Physical. 6.Define(定义)risk management and identify(识别、确定)the four steps in the risk management process. How does enterprise(企业)risk management differ from the traditional form of risk management?(P13.10) Risk management is the process used to systematically(系统地)manage exposures to pure risk. The four steps in the process are ①identify risks, ②evaluate risks, ③select risk management techniques, and ④implement(执行、实施)and review decisions. Traditionally, risk management has dealt primarily(首要地)with pure risks. Enterprise risk management considers all of an entity’s risks(实体风险)together, both pure and speculative(投机的). 8. ABC Company owns 10,000 cars and has determined that it is very likely to suffer between 60 and 70 collision losses this year. XYZ Company also owns 10,000 cars and has determined that it is likely to experience 50 to 80 collision losses this year. Compute the degree of risk for each company, assuming that the companies expect to suffer 65 losses each. (P11) Risk ABC=(70-60)/65=15% Risk XYZ=(80-50)/65=46% 11. Company A owns 100 buildings and averages 2 fires per year. Company B owns 1,000 buildings and averages 30 fires a year. Company A never experiences more than 3 fires a year, although in some years there are none. In some years Company B has as many as 36 fires but never has fewer than 24. Who is faced with the greater objective risk? Who has the greater chance of loss? Explain. (P11) Risk A=(3-0)/2=150% Risk B=(36-24)/30=40% A is faced with the greater objective risk; Probability A=2/100=0.02 Probability B=30/1000=0.03 B has the greater chance of loss. Chapter 2 Risk Identification(识别)and Evaluation(评估) 1. List and briefly describe three methods of identifying risks. (P16-18) One method uses loss exposure checklists(遭损风险核对表)that list various specific sources of loss. Another is the financial statement(财务报表分析)method that involves analyzing each item on a firm’s income statement(损益表)and balance sheet(资产负债表)regarding risks that may be present. A third method uses flowcharts(流程图)to map out the physical flow of goods. Flowcharts can be analyzed with respect to(关于,对于)the types of risks that may affect goods at each point.
保险公司风险管理 一、对企业风险管理概念的理解 近年来,许多学者和国际组织都试图对企业全面风险管理作出全面和权威的定义,较具影响力的国际组织先后给出的定义如下: 风险管理是以文化、过程和结构为基础而驱动企业朝着有效的管理潜在的机会和同时是有效的管理潜在的不利因素的方向发展。 ——AS/NZS4360,1999 风险管理是组织策略管理的核心部分,它是组织以条理化的方式来处理活动中风险的过程,其目的是从每项活动及全部活动的组合中获得持续的利益。 ——AIRMIC/ALARM/IRM,2002 企业风险管理是一套由企业董事会与管理层共同设立,与企业战略相结合的管理流程。它的功能是识别那些会影响企业运作的潜在事件和把相关的风险管理到一个企
业可接受的水平,从而帮助企业达至其目标。 ——COSO-ERM,2004 归纳起来,以上定义基本上基于两个角 度出发:一是从限制不利和促进有利的角度,以澳大利亚/新西兰AS/NZS4360和英国AIRMIC/ALARM/IRM为代表;二是从战略目标 和过程的角度,以美国COSO-ERM为代表。目前,美国的企业往往将COSO-ERM2004的定义视为ERM的定义,而欧盟的企业在相当程度 上将AIRMIC/ALARM/IRM2002视为ERM的定义。现在,ISO层面的ERM概念正在讨论 中,ISO-31000预计将在2009年出台。届时,业界将会有统一的ERM概念。 中国保监会在2007年下发的《保险公 司风险管理指引》中,对风险进行了明确的 定义,即“风险是指对实现保险经营目标可 能产生负面影响的不确定性因素。”保监会在《保险公司风险管理指引》中给出的风险管理定义为:“风险管理是指保险公司围绕 经营目标,对保险经营中的风险进行识别、 评估和控制的基本流程以及相关的组织架构、制度和措施。”
工程项目风险管理与工 程保险 -CAL-FENGHAI-(2020YEAR-YICAI)_JINGBIAN
工程项目风险管理与保险读后感 摘要:在工程项目建设过程中未确知因素、随机因素和模糊因素大量存在,并不断变化,由此而造成的风险直接威胁工程项目的顺利实施和成功。现在,我国工程项目普遍存在投资失控现象,产生这种现象的原因有管理不善和手段落后的原因,更主要的是对影响和制约工程项目的风险因素估计不足,导致在工程项目建设中由风险引起大量的损失。对工程项目的风险加以认识、判断、评价和控制成为一项迫切的任务。 关键词:工程项目风险风险识别识别风险评价 前言:在工程项目管理的各个阶段中,风险的管理应贯彻始终。风险首先是一种不确定性,其次它与损失密切相关,所以从本质上讲,工程风险就是指的在工程建设中所发生损失的不确定性。在工程项目的投标、签约和执行的全过程中,都存在不能预先确定的内部和外部的干扰因素,这种干扰因素可归为工程风险。 近些年,我国有些科研人员对风险管理方法作过一些探讨,但事物总是不断发展变化的,新的方法不断出现,风险管理也日趋完善。对近几年的国内有关风险管理的研究进行回顾,有利于我们总结经验,使我们更好地服务现代化建设。 一、工程项目的风险管理概述 (一)工程项目风险的定义 工程风险管理专家对工程项目的风险定义为:工程项目风险是所有影响工程项目目标实现的不确定因素的集合。 工程项目在其寿命周期中的风险,即工程项目在决策、勘察设计、施工以及竣工后投入使用各阶段,造成实际结果与预期目标的差异性及其发生的概率。项目风险的差异性包括损失的不确定性和收益的不确定性,工程项目风险管理通常研究的是损失的不确定性。(二)工程项目风险的特点 1、风险存在的客观性和普遍性。作为损失发生的不确定性,风险是不以人的意志为转换的客观实在,而且在项目的全生命周期内,风险是无处不在、无时没有的。只能降低风险发生的概率和减少风险造成的损失,而不能从根本上完全消除风险; 2、风险的影响常常不是局部的,某一段时间或某一个方面的,而是全局的。例如,反常的气候条件造成工程的停滞,会影响整个后期计划,影响后期所有参加者的工作; 3、不同的主体对同样风险的承受能力是不同的。人们的承受能力受收益的大小、投入的大小、项目活动的主体的地位和拥有的资源有关;
江西省高等教育自学考试 会计专业本科毕业论文 平安保险公司风险管理研究 论文作者: 准考证号: 作者单位: 指导教师: 主考学校: 完成时间:
目录 一、风险管理概述????????????????????????????????????????????????????????????????????????????????????????????????????????????????????1(一)风险管理的定义????????????????????????????????????????????????????????????????????????????????????????????????????????????1(二)保险公司风险管理概述????????????????????????????????????????????????????????????????????????????????????????????????1二、平安保险风险管理的现状和存在的问题????????????????????????????????????????????????????????????????????????2(一)平安保险风险管理的现状????????????????????????????????????????????????????????????????????????????????????????????2(二)平安保险风险管理存在的问题????????????????????????????????????????????????????????????????????????????????????3 1、保费增长过快的表外风险严重??????????????????????????????????????????????????????????????????????????????????3 2、资产总量高速增长但结构不合理??????????????????????????????????????????????????????????????????????????????4 3、核保核赔制度不完善??????????????????????????????????????????????????????????????????????????????????????????????????5 4、公司部分员工的从业行为不合理??????????????????????????????????????????????????????????????????????????????6 三、加强平安保险风险管理的对策????????????????????????????????????????????????????????????????????????????????????????6(一)强化费率管理避免定价风险????????????????????????????????????????????????????????????????????????????????????????6(二)加强资产风险的管理????????????????????????????????????????????????????????????????????????????????????????????????????7(三)完善核保制度控制承保风险????????????????????????????????????????????????????????????????????????????????????????7(四)加强道德风险的防范与管理????????????????????????????????????????????????????????????????????????????????????????8四、总结??????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????10 参考文献??????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????12
风险管理与保险规划 Document number:BGCG-0857-BTDO-0089-2022
( )1.下列何者属於理财型危险管理方法1危险回避2危险自留3损失抑制4危险预防5专属危险6保险 (A)123 (B)134 (C)256 (D)346 ( ) 2.下列何者为损害填补原则之例外情形1. 定值保险2. 不定值保险 3. 人寿保险 4. 保险单设有自负额条款 5.财产保险 6.定额给 付住院医疗 (A) 1234 (B) 2346 (C) 1245 (D) 1346 ( ) 3.火灾保险契约之转让须经保险人书面同意,因该种保险契约属於: (A)补偿契约 (B)属人契约 (C)附合契约 (D)对价契约 ( )4.保险利益於保险契约订立时,必须存在;但於保险事故发生时,则不必存在,是指下列何者 (A)火灾保险 (B)汽车保险 (C)信用保险 (D)人身保险 ( )5.依照我国保险法的规定,要保人对於下列何者的生命或身体有保险利益
(A)为他人管理财产之人 (B)生活费所仰给之人 (C)债权人 (D)以上皆是 ( )6. 关於投资型保险商品,下列何者正确: I.保险给付随实际投资绩效而定 II.投资型保险商品费用率较共同基金低 III.由被保险人和保险公司共同承担投资风险 IV.保单资讯高度透明化 V.投资型保险商品之保险给付要缴所得税 (A) I, II, III (B) III, IV (C) I, IV, V (D) I, IV ( )7.下列何者具有保险利益 (A)已私订终身之同居男女朋友互有保险利益 (B)已出嫁的女儿对生父或生母有保险利益 (C)订婚之男女朋友互有保险利益 (D)以上皆是 ( )8.保险人行使代位求偿权之金额,以下列何者为限 (A)侵权行为人法定赔偿金额 (B)保险契约之保险金额 (C)保险人之赔偿金额 (D)被保险人之投保金额 ( )9.因财产毁损而花费之修理复原费用,属於下列何项损失 (A)间接损失 (B)直接损失 (C)从属损失 (D)责任损失
平安保险公司风险管理浅研 摘要 随着新经济时代的来临和人们生活水平的提高,国民需求已经发生了极大的变化,人们不再担心温饱的问题,所以,保险在人们心里的地位日益提高,保险的重要性也越来越大。我国很多保险公司在对公司整体的风险管理上仍然有很多问题,存在着许多重大的漏洞。如今中国的保险公司日益发展,很多国内的保险公司越做越大,但是公司越做越大,随之而来的是一系列的问题,缺少自我风险管理的能力,本文在对中国保险公司的领头羊中国平安保险的风险管理概念解析的基础上分析了我国平安保险公司实施风险管理的重要性,针对我国平安保险公司风险管理中存在的问题提出了相关对策。 关键词:平安保险风险管理企业发展 近年来,我国不断改进保险监管和实践,加强对保险消费者利益的保护,保险市场持续健康发展。据统计,我国保费收入世界排名由2010年的第6位上升至2012年的第4位。中国保险机构作为发展中国家的唯一代表入选G-SII是我国保险业积极参与国际金融治理、维护全球金融稳定的重大举措,体现了国际社会对我国经济金融改革与发展成就的充分肯定,也是对我国保险业在国际保险市场上影响和地位的认可。面对保险行业的发展日益国际化,我国保险公司只有加强风险管理才能在国际的大围环境下健康快速的发展。 一、保险公司风险管理概述 1、保险公司的风险管理包括风险识别、风险分析和风险衡量
通过风险源的识别可以分析出保险公司所面临的外部环境风险,通常包括物质环境风险、社会环境风险、政治环境风险、法律环境风险、技术环境风险、经济环境风险、金融环境风险等几个方面,它们是保险公司风险管理的重要组成部分,因其来自外部,我们称之为非保险风险;通过风险标的的识别可以认识到保险公司的主要受损标的是金融资产还是人力资本;通过识别各个经营环节风险可能造成的损失可以明确保险公司的销售、承保、定价、理赔及投资风险与危害之间的关系,从而形成了保险公司的内部经营风险。对于保险公司而言,风险造成的最大危害就是企业破产,除此之外,风险还会使保险公司实际收益与预期收益发生偏离从而蒙受损失或丧失额外收益,这种结果也是保险公司的危害。从危险因素入手,保险公司可以结合保险经营各环节进行风险分析。通过风险衡量,计算出较为准确的损失概率,可以使保险公司在一定程度上消除损失的不确定性。对损失幅度的预测,可以让保险公司了解风险所带来的损失后果,进而集中力量处理损失后果严重的风险,对保险公司影响小的风险则不必过多投入,如可以采用自留的方法处理。 2、保险公司的风险管理方法包括损失控制和损失融资 所谓损失控制,是指企业对不愿放弃也不愿转移的风险,通过降低其损失发生的概率,缩小其损失发生的程度来达到控制目的的各种控制技术或方法。损失控制的目的在于积极改善风险单位的特性,使其能为企业所接受,从而使企业不丧失获利机会。制定损失控制措施必须以定量风险评价的结果为依据,才能确保损失控制措施具有针对性,取得预期的控制效果。风险评价时特别要注意间接损失和隐蔽损失。损失融资指在意外事件发生时通过获取资金而支付或抵偿损失。它的主要措施包括自留、保险以及以合同方式将损失转由保险公司以外的其他人承担。在大中型公司中往往都有一个正式的损失融资计划。通过购买保险合同降低风险是另一种选择。按保险合同要求公司向保险公司支付保险费,当有符合合同条款的损失发生时保险公司为规定的损失支付资金。保险合同降低了购买保险一方的风险,它把损失转嫁给了保险公司,而保险公司则是通过损失分摊的原则降低自己的风险。 一、平安保险风险管理的现状
保险公司风险管理 根据《保险公司风险管理指引(试行)公司将风险定义为对实现保险经营目标可能产生负面影响的不确定性因素。公司参照该指引借鉴国际现行的风险分类方法,同时考虑到公司的实际情况将风险分为定性风险和定量风险两大类,具体分类如下: 一、定性风险 (一)战略风险指由于战略决策或发展规划错误给公司业务带来不利影响的风险。(二)声誉或品牌风险:由于客户对公司的不良印象而对经营造成不利影响导致的风险。 二、定量风险 (一)保险风险指由于死亡率、疾病率、赔付率、退保率等判断不正确导致产品定价错误或者准备金提取不足,再保险安排不当,非预期重大理赔等造成损失的可能性。 (二)市场风险是指由于利率、汇率、权益价格和商品价格等市场价格的不利变动而造成的损失,以及由于重大危机造成业务收入无法弥补费用的可能性。 市场风险可以分为: 利率或资产负债匹配风险:指由于利率的变动给公司造成损失的风险。 权益风险指:由于股价的变动给公司造成损失的风险。 汇率风险指:由于汇率的变动给公司造成损失的风险。 商品风险指:由于商品价格变动给公司造成损失的风险。 流动性风险指:由于面临到期支付时持有的资产流动性差和对外融资枯竭而造成损失或破产的可能性。 (三)信用风险是指由于债务人或者交易对手不能履行合同义务,或者信用状况的不利变动而造成损失的可能性。 违约风险:指不履行按合同所承担的义务,给公司造成损失的风险。 利差风险:指由于与基准的差异发生变化,导致价值的波动给公司造成损失的风险。 迁移风险:指由于信用级别的变化,引起价值的波动,给公司造成损失的风险。 再保风险:指再保险公司信用级别的变化以及不能履行合同所承担的义务而给公司成损失的风险。 (四)商业风险指在重大危机过后,保险业务的未来的收入不能覆盖未来的费用——不包括这些已经被其他种类风险所包含的费用和收入项目。商业风险是由于人们对未来可能发生的费用、已经存在的商业竞争(持续性)和未来如何重新定价的不确定而引起的结果与预期之间的偏差。 (五)操作风险指由于操作流程不完善、人为过错和信息系统故障等原因导致损失的可能性。
保险公司流动性风险管 理报告 Standardization of sany group #QS8QHH-HHGX8Q8-GNHHJ8-HHMHGN#
XX保险股份有限公司 流动性风险管理半年度报告(模板) 201X年X月 一、流动性风险管理的基本情况 (一)流动性风险管理的组织架构与履职情况 参考示例: 流动性风险是指公司无法及时获得充足资金或无法及时以合理成本获得充足资金,以支付到期债务或履行其他支付义务的风险。公司目前主要面临……等流动性风险。 公司按照分工明确、相互制衡原则,已建立由董事会承担最终责任,董事会风险管理委员会、总裁室、计划财务部、投资管理部、产品精算部、战略企划部等相关部门构成的流动性风险管理体系。其中,计划财务部负责定期评估公司流动性风险水平及管理状况,向董事会风险管理委员会定期汇报公司流动性风险状况,及时汇报流动性风险的重大变化或潜在转变。计划财务部与产品精算部负责执行公司的相关政策、策略和程序,组织实施压力测试和情景分析,并定期将测试结果向总裁室、风险管理委员会及董事会汇报,推动压力测试成果在战略决策和风险管理中的应用。 ……
(二)流动性风险管理制度建设与改进情况 参考示例: 公司于201X年X月至X月期间,拟定了《XX保险股份有限公司流动性风险管理办法》和《XX保险股份有限公司流动性风险应急预案》,明确了流动性管理总体目标和管理原则,并制定了流动性风险管理机制。 流动性风险管理的基本目标,是在满足客户支付结算、公司日常经营、偿还债务的前提下,保持合理的流动性水平,科学配置资产负债,最大限度地减少因流动性原因产生的支付风险及突发事件给公司造成经济损失,维护广大客户的利益,确保公司稳健发展。公司根据业务规模、产品结构、风险状况及场环境等因素,在充分考虑其他风险对流动性风险的影响和公司的整体风险偏好的基础上,确定了201X年度流动性风险偏好和容忍度。 (三)当期的重大流动性风险事件描述、成因分析与应对措施(如有) 参考示例: 公司目前处于快速发展时期,新业务保费每年流入较多,即使不考虑存量资产的到期现金流以及通过回购融入现金的能力,也足以支持保险赔付支出,面临的流动性风险较小。在基本情景下的压力情景测试结果显示,公司的净现金流无论现在或未来都为正值,公司可以保证现金的流动性,满足业务量的持续上升。
浅析保险公司内控合规管理工作 由于保险市场与资本市场、货币市场的密切关系,保险公司所需要面临的巨大风险也不言而喻。这些风险复杂难测,涉及自然灾害、意外事故,且日益受到投资环境、货币政策等风险因素的影响。因此,我们保险公司应切实研究风险方法的措施与途径,积极防范和化解内部及外部风险。内部控制是保险公司防范风险的第一道防线,处于基础性地位,因此强化内部控制能力是我们完善内部控制系统的首要任务。 一、内控的内涵及国内保险企业内控现状. (一)什么是内部控制 内部控制指的是“企业防止舞弊的工具”①。《独立审计具体准则第9号一内部控制与审计风险》中对内部控制作了定义:“本准则所称内部控制.是指被审计单位为了保证业务活动的有效进行.保护资产的安全和完整,防止、发现、纠正错误与舞弊,保证会计资料的真实、合法、完整而制定和实施的政策与程序。内部控制包括控制环境、会计系统和控制程序。 (二)国内保险企业内部控制现状 纵观中国保险公司内部控制演进步程,国内保险企业内部控制建设终究是取得了一定的成效,但总体上内部控制环节仍旧比较薄弱.内控功效表现紊乱、机制失衡,从而引发行业内的经济犯罪和经营失误屡见不鲜,与国际上保险行业内部控制水平依旧存在较大差 ①出自《独立审计具体准则第9号一内部控制与审计风险》(会协字〔1996〕456号)1996.12.26出版
距: 1.保险公司内部控制建设的动力不足 在中国保险行业内部控制发展的过程中,来自保险公司外部的推动因素作用一直都有着举足轻重的作用,而保险公司内部自身强化建设的意愿较弱。国外监管市场存在着一句名言:“如果将外部监管变成金融机构内控不足的步补充,风险的悲剧就会不断上演。”金融机构的内部控制是金融市场健康运行的基础和前提,即便是有效的外部监管和监督都无法替代金融机构的自我约束及自我内部控制。 回顾中国保险公司内部控制的发展史,中国监管部门对保险公司内部控制建设的影响实为突出,是推动中国保险公司内部控制建设的关键因素。随着中国保险监督管理委员会有关行政法规地不断颁布,依托监管部门的监督,保险公司逐渐正确认识和着手内部控制建设工作。同时,中国保险公司在参与国际资本市场的过程中,迫于国际资本市场监管的压力,内部控制水平也得到了大幅提升。 监管部门的作用如若愈是突出,愈能证明保险公司自身内部控制动力上的欠缺及乏力。对部分保险公司而言,内部控制建设是否达到监管部门的要求,也许比内部控制是否在公司实际经营过程中发挥作用更为重要。 2.内部控制体系不健全,制度建设滞后于业务发展 根据COSO报告,保险公司内部控制体系包括五大要素,即控制环境、风险管理、控制活动、信息与沟通及监督,这些要素存在于保险公司经营活动的各方各面,。很大部分的保险公司在控制活动方面制定了较多措施与制度,但仍存在精细化程度不高、深入化程度不够的问题,未能渗透到公司各项业务活动的各个操作环节,也未能覆盖
浅析保险公司风险管理
广东金融学院 学年论文 论文题目浅析保险公司风险管理 学生姓名郭志河学号 081532153 专业班级风险管理与精算 指导教师袁建华职称副教授 2011 年 6 月23 日
摘要 保险公司风险管理是对风险的识别、衡量和控制的技术方法,其目的是直接有效地推动组织目标的实现。风险管理包括风险识别、风险分析和风险衡量。目前,我国保险公司风险管理呈现以下现状,如寿险公司业务核保不完善,承保风险突出;费率厘订过于标准化;投资风险表现突出;资产总量增长但结构不合理;核保核赔制度不完善等。针对内部经营风险可以采取加强资产风险的管理,完善核保制度,强化费率管理等方法。针对外部风险可以采取转变经营思路,加快培养人才,积极调整产品结构等方法。在经济全球化、金融一体化迅猛发展的今天,保险公司所面临的风险越来越大,我国保险公司应当从物质和观念上为今后在中国保险业全面推行综合风险管理做好充分的准备。 关键词:保险;风险管理。
目录 一、保险公司风险管理的内容及方法 (1) (一)风险管理的内容 (1) (二)风险管理的方法 (2) 二、我国保险公司风险管理现状分析 (4) (一)我国寿险公司内部经营风险主要表现 (4) (二)我国产险公司内部经营风险主要表现 (4) 三、提高我国保险公司风险管理水平的措施 (6) (一)针对内部经营风险采取的措施 (6) (二)针对外部经营风险采取的措施 (7) 四、我国保险公司风险管理未来发展的方向 (8) 参考文献 (10)
一、保险公司风险管理的内容及方法 (一)风险管理的内容 保险公司风险管理是对风险的识别、衡量和控制的技术方法,也可以指经济主体用以降低风险负面影响的动态连续过程,其目的是直接有效地推动组织目标的实现。保险公司风险管理的总体目标是实现企业价值最大化,企业价值最大化将通过风险成本最小化实现。 1.保险公司的风险管理包括风险识别、风险分析和风险衡量。 保险公司的风险识别应从风险源、受损标的、危害及危险因素四个方面入手: (1)通过风险源的识别可以分析出保险公司所面临的外部环境风险,通常包括物质环境风险、社会环境风险、政治环境风险、法律环境风险、技术环境风险、经济环境风险、金融环境风险等几个方面,它们是保险公司风险管理的重要组成部分,因其来自外部,我们称之为非保险风险; (2)通过风险标的的识别可以认识到保险公司的主要受损标的是金融资产还是人力资本; (3)通过识别各个经营环节风险可能造成的损失可以明确保险公司的销售、承保、定价、理赔及投资风险与危害之间的关系,从而形成了保险公司的内部经营风险。对于保险公司而言,风险造成的最大危害就是企业破产,除此之外,风险还会使保险公司实际收益与预期收益发生偏离从而蒙受损失或丧失额外收益,这种结果也是保险公
Value Engineering 当今经济竞争是如此的激烈,不确定因素在不断的增加,给工程项目带来了各种风险,因此,风险管理和保险在项目管理中受到普遍的重视。 1风险管理 随着我国经济的快速发展,工程项目必然向规模大、难度高、材料新颖、施工工艺要求高等方面发展,工程项目管理的重要性越来越明显。而我国的项目管理经验不足,与发达国家的管理水平有一定的差距。本文结合国际项目管理中的风险管理做一简单的论述。 1.1工程项目风险的概念。(1)什么是风险?事先不能确定的内部和外部的干扰因素,就是风险。(2)什么是风险管理?风险管理就是人们对潜在的意外损失进行识别、评估,并根据具体情况采取相应的措施进行处理,即尽可能有备无患或在无法避免时亦能寻求切实可行的补救措施,从而减少意外损失或进而使风险为我所用。(3)为什么要风险管理?一项工程的工期长、参与方多、易受外界影响,这样就会导致成本增加,利润减低,甚至有可能使项目失败。这样的案例在我国是很多的,结果造成大量的资源浪费。 1.2工程项目风险的特点。(1)风险的客观性与必然性。在整个工程项目中,风险的存在与发生,总体而言是一种必然现象。(2)风险的多样性。在一个工程项目中有许多种类的风险,如自然风险、政治风险、合同风险、经济风险等,这些风险之间又有复杂的内在联系。(3)风险在整个项目生命期中存在,而不仅仅是在实施阶段。如:在设计阶段,可能存在专业不协调、地质不确定、图纸错误等;在施工阶段,可能存在物价上涨、资金缺乏等。(4)风险影响全局性。如:气候异常导致工程停滞,带来了工期的延长,同时也增加了费用。一个活动受到风险干扰,可能影响到与它相关的许多活动,因此,在工程项目中的风险影响,随着时间推移有扩大的趋势。(5)风险有一定的规律性。工程项目的环境变化、项目的实施有一定的规律性,所以,风险的发生和影响也有一定的规律性,是可以预见的。需要管理人员要有风险意识,重视风险,对风险进行全面的控制。 1.3风险管理中常有的应对方法。(1)风险回避。风险回避是一种消极的风险处置方法,再大的风险也只是可能发生,也有可能不发生。采取回避,当然是能彻底消除风险,但同时也失去了可能的收益。应该根据自身特点,回避风险大的,选择风险小或者适中的。(2)风险减轻。对损失小、概率大的风险,可采取控制措施来降低风险发生的概率,对于风险已经发生的,要采取措施尽可能的减少损失。风险控制与风险回避不同,风险控制是一种积极、有效的处理方式,它能有效地减少项目因风险事件而造成的损失。(3)风险保留。对损失小、概率小的风险留给自己承担,要主动承担风险,而不是被动承担,被动承担往往造成严重后果,使项目遭受重大的损失。(4)风险预防。风险预防有汇率风险的预防、技术风险的预防、合同风险的预防。通常风险预防采用技术措施或管理措施来防止不确定因素的出现或者减少已经出现的因素,降低风险发生的概率,做到防范于未然。(5)风险转移。风险转移又分为保险风险转移和非保险风险转移。保险风险转移在国外是很常见是事,但在国内的案例不多,主要是由于管理人员对风险的意识淡薄。 非保险风险转移有:担保合同、租赁合同等。通过合同转移风险在国内外都很普遍,通过合同可以降低个体的风险。但要选择信誉好、能力强合作伙伴。 2工程保险 在国际中,投保是应对风险的一种重要手段和普遍做法。随着我国经济的快速发展和工程建设的需要,以及我国管理人员对风险意识的不断增强,参与保险的项目会越来越多,工程保险市场前景广阔,在此介绍一下国际工程中使用的保险。 工程保险是以承保建筑为主体的工程,在整个建设期间,由于保险责任范围内的风险给工程项目造成损失而提供经济赔偿保障的保险。 2.1工程保险的特征有:(1)承保风险的特殊性。工程保险承保的项目绝大多数是在风险中,同时,工程施工工程中始终处于动态的,各种风险相互联系,使得风险程度增加。(2)风险保障的综合性。工程保险既承担财产损失的风险,又承担责任风险,还可以根据工程项目情况承担其他风险。(3)投保人具有广泛性。可以是业主,也可以是承包人,任何一方都可以投保。 2.2工程保险的分类:(1)综合工程险。主要针对因自然灾害和意外事故造成的财产损失和依法应对第三人人身伤害所承担的经济赔偿责任提供保障的一种综合性保险。(2)雇主责任险。主要是保护业主和承包商的雇员遭受工伤时雇主应承担的责任而设立的保险。(3)工程延误及预期损失险。是针对因自然灾害和意外事故导致工程不能按期交付,并由此造成预期收益损失提供的保险。(4)工程质量保险。是针对承包商为保证工程完工后出现的质量缺陷进行修理、弥补、赔偿提供可靠的资金保障的保险。(5)货物运输险。此保险包括海洋运输保险、路上运输保险等。(6)施工机具险。是对施工机具在使用或停放过程中,因自然灾害或意外事故造成的损失提供的保险。(7)雇员忠诚险。主要是弥补因雇员的欺骗或不忠行为而给项目造成损失设立的保险。(8)职业责任险。与工程项目关系最大的是设计责任险,主要的承担设计人员在设计过程中的疏忽、过失而引发的工程事故,造成工程本身的经济损失和产生的诉讼费用。在国际中,设计公司常常为设计师投保,有些国家的行业协会,强制要求为技术人员投保职业责任险。(9)履约保障险。针对因承包商自身的错误导致合同不能履行时,为保障业主及时聘请其他承包商继续施工所提供的保险。 总之,风险管理与保险是现代工程项目管理中必不可少的一项工作,通过剔除风险以减少成本,从而给业主带来更多的经济效益,最大限度地实现业主的建设目标。 参考文献: [1]李慧民.工程项目管理[M].北京:中国建筑工业出版社. [2]李慧民.建筑工程经济与项目管理[M].北京:冶金工业出版社. [3]全国二级建造师职业资格考试用书.建设工程施工管理[M]. [4]雷胜强.国际工程风险管理与保险[M].北京:中国建筑工业出版社. 建设工程项目风险管理与保险 On the Risk Management and Insurance of the Construction Project 王清波Wang Qingbo (泉州市建设系统培训中心,泉州362000) (Quanzhou Building System Training Center,Quanzhou362000,China) 摘要:在我国的许多项目中,由于没有风险意识而造成的损失是巨大的,同样,风险和盈利是同时存在的,通常风险大的工程项目才有较高的盈利,降低风险的目的就是减少不必要的成本开支,以实现目标利润,创造良好的经济效益。这样,风险管理就成为项目管理的重点之一。 Abstract:In many of the programs in our country,the losses are great due to the lack of risk awareness.Both the benefits and challenge exist.Risky projects often have higher earnings,lower risk is the objective of reducing unnecessary costs to achieve target profit,to create a good economic benefits.In this way,risk management has become one of the key project management. 关键词:工程项目风险管理;经济效益;应对方法;工程保险 Key words:the risk management of construction;economic benefits;measures;project insurance 中图分类号:TU723文献标识码:A文章编号:1006-4311(2010)04-0163-01 ·163·
保险公司风险管理 据瑞士Sigma统计,从1978—1994年16年间,世界上有648家保 险公司破产,尤其是1996—2001年,保险业高度发达的日本连续7 家生命保险公司破产。在我国,标准普尔在《中国保险业信用前瞻2006—2007》中对我国保险业风险的评价是:无论寿险还是非寿险的 行业风险依然较高。这给我国保险业敲响了警钟:保险公司在经营风 险产品的同时,必须增强自身的风险管理。美国反舞弊财务报告委员 会的发起组织委员会(COSO)发布的企业风险管理框架提出的全新的风 险管理理念和技术对于我国保险企业的风险管理具有极大的理论和实 践意义。 一、保险企业实施全面风险管理的必要性和重要性 保险公司的风险管理是一个永恒的话题,保险公司围绕总体经营目标,通过在企业管理的各个环节和经营过程中执行风险管理的基本流程, 培育良好的风险管理文化,建立全面风险管理体系,可以起到防范和 化解风险、保护资产的安全与完整、保证经营活动合法合规和企业经 营战略有效实施等重要作用,因此,是否实施全面的风险管理是衡量 保险企业经营管理水平高低的重要标志。 (一)保险国际化的趋势日益明显 在经济全球化的大背景下,保险国际化的趋势日益明显,一方面表现 为客户保险需求的全球化,跨国公司基于其全球经营业务在世界范围 内安排其风险管理与保险计划;另一方面表现为保险人通过国际间的
保险资本运作、对冲机制、战略联盟等多种形式,满足巨灾保险、金融风险管理等迅速增长的需求,在国际范围内寻求新的生存和发展空间。20世纪60年代出现的真正意义下的自保公司,70年代由荷兰人首创并迅速风靡全球的银行保险,80年代人寿保险业出现的以万能寿险和变额寿险为代表的产品创新,90年代出现的保险风险证券化以及大量新型风险转移工具,特别是近年来,处于前锋地位的保险人、保险经纪人、政府保险机构及民间保险组织,如安联保险等,已经在综合风险管理(IntegrateRiskManagement)、非传统风险转移工具(AlternativeRiskTransfers)等新型保险产品和技术等方面进行了大量的创新,保险保障的范围已经大大突破了传统意义上的可保风险范畴,从而预示着未来保险业的革命性变化。 (二)保险资金面临的投资风险越来越大 随着金融市场的创新与融合,保险资金运用渠道的逐步拓宽,可投资品种逐步增加,从普通的债券投资发展到权益类投资、从国内市场拓展到境外市场,保险资金特别是寿险业资金面对的各种风险也越来越复杂。例如,寿险保单存续期一般都长达20至30年,相对应的在资金运用中要考虑20-30年存续期的投资与之相匹配。投资于固定收益资产的寿险资金,对利率的变动非常敏感,市场利率的微小波动会导致资产价值的较大变动。据统计,到2006年8月,债券已经成为保险资产配置的最主要工具,投资规模已经达到8777亿元,其中,持有国债和金融债余额分别达到3674亿元和2416亿元,债券资产占保险资产运用的比重由2001年的28.4%上升到2006年的55.2%,保险公司